The different roles of flag state authorities, insurers, crewing agencies, seafarers and ship-owners influence the way they look upon risk in the context of medical selection. While all share common objectives like safety for ship and crew, they vary in the emphasis they put on other aspects, like rights to work, safety of operation, loss prevention, flag reputation etc. The drivers for development of criteria development differ. Hence, the criteria also differ.
The objectives of the health assessment define the mind-set of the medical examination, and the approach of the medical examiner. The medical examiner could interpret a criterion differently under different mind-sets and objectives.
Regardless of type of PEME programme, the need to use a heuristic approach and the limits of evidence-based criteria are striking. We have to face this challenge in the future.
C.8.5 Negative v Positive selection
Details
ALF MAGNE HORNELAND
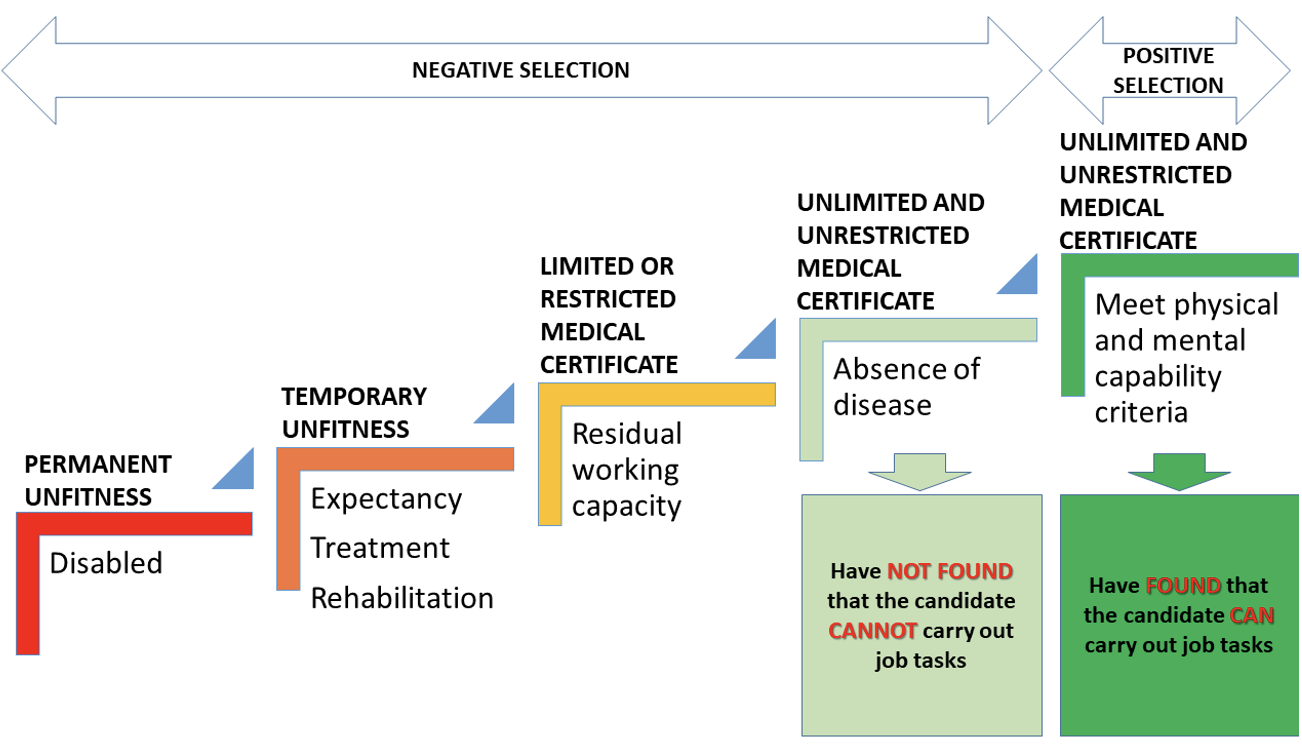
There are important differences between negative and positive selection. The starting point is a healthy individual, suffering from no known medical condition. Whilst the negative selection focus on finding something that is medically ‘wrong’ with the individual – i.e. any medical diagnosis, the positive selection focus on assessment of the performance of the individual, both cognitive and physical performance.
Negative selection
This is the most common method for medical selection in civil life. As a starting point, the medical examiner regards the candidate as fit for duty if he is not suffering from a medical condition, a disease, sequelae from a medical incident or earlier disease, or is disabled due to a medical condition.
The examination ‘rules out’ those people with defined medical diagnoses (also including reduced vision and hearing) at a prescribed cut-off point. Those who are not ‘ruled out’ are regarded as ‘ruled in’. The conclusion is that you have not found that the candidate cannot carry out his job tasks; therefore, he is, per definition, fit for work.
Most of the PEME schemes focus on negative selection, less on positive selection. The detailed list of medical conditions in the international guidelines emphasizes this fact.
Positive selection
At the point where negative selection concludes, positive selection starts. All those who are regarded as fit after negative selection, are in principle again regarded unfit for work, unless they demonstrate certain minimum capabilities. Where the negative selection is concerned about medical diagnoses only, the positive selection focus on physical and mental capabilities.
Sometimes vision and hearing also are included in the positive selection scheme. It is, however, hard to argue that a better vision than Snellens decimal notation 1.0 is needed, or that a hearing better than what is regarded “normal” (meaning the ability to hear pure tones of 20 dB or lower) is needed in any particular job position. Hence, it is my personal opinion that assessment of visual and hearing capacities are to be regarded as parts of negative selection.
This type of selection is common in selection for service in the military, in a fire brigade, as police officers and some other physically and/or mentally demanding professions.
In seafaring, the PEME also includes aspects of positive selection, but only to a certain extent. It is usual to carry out cognitive or psychometric tests in many clinics, mainly in the typical crewing countries and mainly du to enhanced PEME requirements. However, at present there is no evidence that demonstrates the validity of carrying out such tests, whether they are fit for purpose or not[1]. The diversity of jobs on board ship makes it difficult to design a physical or a mental test that actually corresponds to the job tasks the candidate is going to carry out in his profession. Hence, it is wise to be careful regarding recommendations of specific physical, cognitive or mental tests and define cut off points for inclusion or exclusion of the candidate.
The table B-I/9 of the STCW Code[2] lists the minimum tasks a seafarer must manage, and the corresponding physical and cognitive capacity. There is also a third column, listing what the medical examiner should verify, but it has a general form, that makes the advice quite woolly.
The diversity of jobs and job tasks on board, call for a differentiation in testing procedures, should one decide to give advice that is more detailed. To be sure that the tests are actually ‘ruling in’ those who have the necessary capacity, the cut-off point of the criterion needs to be sufficient. To avoid that people with the sufficient capacity are not ‘ruled out’, the cut-off point of the criterion also needs to be necessary. Today’s medical examination schemes for pre-employment examinations, regardless of industrial sector or profession, rarely meet these requirements.
The illustration below (Figure 1) shows the connection between negative and positive selection.
Figure. 1. Relation between negative and positive selection. This model has been used in training of seafarers’ doctors by the NCMDM since 2009 – latest revision 2019
References
[1] ILO/IMO Guidelines on the medical examination of seafarers. Section XII Conduct of medical examinations (xi). Page 12.
[2] International Convention on Training, Certification and Watchkeeping for seafarers, STCW Code, Part B, Table B-I/9.
C.8.3 Rights to work - antidiscrimination aspects
Details
ALF MAGNE HORNELAND
Medical selection inevitably involves differential treatment of individuals. Some will be allowed to work in a specific position or profession, while others will be denied.
The Universal Declaration of Human Rights (UDHR), adopted in 1948 by the United Nations general Assembly, is now regarded as well-established international law in most countries, whereas other countries disagree, like Saudi-Arabia[1] and Iran[2]. The US Supreme Court limited the effect of international law in one case regarding the Alien Tort Statute and concluded that the Declaration “does not of its own force impose obligations as a matter of international law”[3]. At the time of adoption, eight countries abstained[4] (Czechoslovakia, Poland, Saudi Arabia, Soviet Union, Byelorussian SSR, Ukrainian SSR, South Africa and Yugoslavia), and two countries did not vote (Honduras and Yemen). The UDHR was the first international convention to establish a ‘right to work’[5] internationally, and is binding for member states, according to the UN Charter. It was the first step towards the establishment of the International Bill of Human Rights, which, in addition to the UDHR, also contains the International Covenant on Civil and Political Rights (ICCPR)[6] and the International Covenant on Economic, Social and Cultural Rights (ICESCR)[7] of 1966. Similar regional charters have been agreed in different areas of the world[8][9].
The right to work now seems to be well established internationally, although implementation in national law and compliance vary considerably around the world.
The individual’s right to work primarily is an obligation of the government to establish rules and framework that ensures that people, even if they have a disability, shall have opportunities to have a job. The UN Convention on the rights of persons with disabilities[10] elaborates this in more detail, emphasizing that they shall enjoy full equality under the law. The ILO further focused on the issues in the Vocational Rehabilitation and Employment (Disabled Persons) Convention, 1983 (No. 159).
The right to work for people with disabilities and the minimum requirements for medical fitness of workers sometimes can be seen to challenge each other.
The lawful differential treatment of workers, according to Norwegian legislation[11] reads (bold types by the author):
“Section 9. Lawful differential treatment
Differential treatment does not breach the prohibition in section 6 if it:
a) has an objective purpose,
b) is necessary to achieve the purpose, and
c) does not have a disproportionate negative impact on the person or persons subject to the differential treatment.
In employment relationships and in connection with the selection and treatment of self-employed persons and hired workers, direct differential treatment on the basis of gender, ethnicity, religion, belief, disability, sexual orientation, gender identity or gender expression is only permitted if the characteristic in question is of decisive significance for the performance of the work or the pursuit of the occupation and the conditions in the first paragraph are met.”
The last sentence is a long and complicated one, which regards more than assessment for the ability to work. The bold types make it clearer: “In employment relationships, … direct differential treatment on the basis of … disability … is only permitted if the characteristic in question is of decisive significance for the performance of the work…”
The ‘objective purpose’ is not the tripwire in this context. Most medical fitness standards and criteria have an objective purpose.
It is far more challenging to establish the evidence underpinning the necessity to meet a specific criterion to be able to carry out a specific task or job on board ship. The lack of evidence for setting such a cut-off point for any criterion, is striking. Most pre-employment medical examinations are carried out in a heuristic way (see below), i.e. in a practical way, without ability to demonstrate that it is evidence based, even if it is regarded sufficient for issuing a medical certificate. The sound judgement of the medical examiner often has no other substantiation than a gut feeling, with reference to some rules that also lack evidence for their appropriateness, other than that of expert consensus.
Although statutory PEME schemes probably will not be regarded as discriminatory, the assessment in a single case could violate anti-discrimination principles. According to these principles, referred above, the need to deny someone a medical certificate should not only be sufficient for the objectives of the PEME scheme, rather also necessary. A decision that meet only the sufficient criterion could be far stronger than what is necessary – it would still be sufficient. On the other hand, what is regarded to be necessary, not always is enough to be sufficient! This is the dilemma of the medical examiners: Both criteria should be met at the same time.
How this could apply to the single decision by a seafarers’ doctor, is illustrated by a case for the Norwegian Anti-Discrimination Tribunal in 2019[12] (see frame).
Norwegian Anti-Discrimination Tribunal - Case No. DIN-2019-440
The Norwegian Anti-Discrimination Tribunal decided that the decision by a seafarers’ doctor to declare a seafarer unfit, was an unlawful direct discriminatory decision because:
The doctor based the decision on the diagnoses HIV+, hepatitis C and syphilis without assessing whether the condition of the seafarer was of decisive significance for performing job tasks. All these conditions can, according to the regulations, lead to temporary or permanent unfitness.
The tribunal concluded:
«Whether provisions for lawful differential treatment are met, must be considered in the particular case. Hence, it is not decisive that the ‘Regulations on medical examination of employees on Norwegian ships and mobile offshore units’, lay down the general principle that differential treatment because of disability can be lawful, necessary and reasonable.»
The practice may be different in other countries, e.g. in UK and Canada where it is more likely that the authorities will be held accountable for discrimination provided the doctor followed the published standards[13].
Seafarers’ medical examiners should be aware of those issues. In principle, nobody should be denied working on board without an individual risk assessment in relation to the specific tasks and the specific job tasks the seafarer is going to have on board the ship. The medical examiner should bear in mind that being too strict, could violate the human rights to work, whilst being too lenient could violate the obligations to be able to work on board, as well as the safety of ship, crew and self. The result could be delays, diversions, risky evacuations, hospitalisations, repatriations, replacements of crew – and the costs relating to these matters.
References
[1] Nisrine Abiad (2008). Sharia, Muslim states and international human rights treaty obligations: a comparative study. BIICL. pp. 60–65. ISBN 978-1-905221-41-7.
[2] Littman, D (February–March 1999). "Universal Human Rights and Human Rights in Islam". Midstream. Archived from the original on 2006-05-01.
[3] United States, the Supreme Court in Sosa v. Alvarez-Machain (2004)
[4] "Yearbook of the United Nations 1948–1949 p 535" (PDF). Archived from the original (PDF) on September 27, 2013. Retrieved 24 July 2014.
[5] Universal declaration of human rights, article 23.1
[6] International Covenant on Civil and Political Rights (ICCPR), adopted by the United Nations General Assembly. Resolution 2200A (XXI) on 16 December 1966, and in force from 23 March 1976
[7] International Covenant on Economic, Social and Cultural Rights (ICESCR) adopted by the UN General Assembly on 16 December 1966, in force from 3 January 1976.
[8] African Charter on Human and Peoples’ Rights, Organisation of African Unity
[9] Convention for the Protection of Human Rights and Fundamental Freedoms, or European Convention on Human Rights (ECHR) of 4 November 1950, in force from 2 September 1953
[10] Convention on the Rights of Persons with Disabilities (CRPD), signed 23 March 2007, effective from 3 may 2008
[11] Act relating to equality and prohibition against discrimination (Equality and Anti-Discrimination Act) of 16th June 2017, No. 51.
The APA Dictionary of Psychology defines a heuristic as follows:
In cognition, a heuristic is an experience-based strategy for solving a problem or making a decision that often provides an efficient means of finding an answer but cannot guarantee a correct outcome. By contrast, an algorithm guarantees a solution but may be much less efficient. Some heuristics, such as the availability heuristic or representativeness heuristic, involve systematic bias, also called cognitive heuristic.[1]
Because they rely on less information, heuristics are assumed to facilitate faster decision-making than strategies that require more information. Seafarers’ doctors make decisions several or many times a day and probably use a heuristic approach most of the time. An evidence-based approach often would be more time consuming, although not necessarily.
The evidence basis for medical fitness standards and criteria
The level of scientific evidence that forms the basis for decision-making regarding medical fitness criteria and their cut-off points is that of ‘expert consensus’, i.e. the lowest possible level of evidence according to Oxford centre for Evidence-based Medicine[2][3]. Adjustments have been made throughout their 100-year history several times, taking into account the experience of practising the standards and criteria. Today we probably can conclude that the criteria and their cut-of-points are ‘sufficient’, but it probably would be hard to argue that they always are ‘necessary’.
The Guidelines on the medical examination of seafarers from ILO and IMO were developed in a series of tripartite meetings[4] between employers’ organisations, employees’ organisations and government representatives, under the leadership of ILO and IMO. Eight Government experts nominated by IMO, four ship-owner and four seafarer representatives nominated by the respective groups of the ILO’s Joint Maritime Commission attended the tripartite meetings. Several other government representations also participated, along with a number of observers from intergovernmental and non-governmental organizations[5]. The meeting reached their decision by consensus, which mean that they had to compromise. Scientific medical evidence was just one ingredient, the others being political, financial, and legal as well as party interests. It is therefore difficult to claim that it is ‘necessary’ to meet these criteria to accomplish the job tasks for a given seafarer. We also need a definition of ‘necessary’ in this context.
However, in lack of a better option, expert consensus is the best we can get, and without compromises and consensus, there would be no international recommendations for minimum health requirements for seafarers, leaving us with a wilderness of less substantiated and less useful requirements.
Colour vision requirements[6][7] is one example that is difficult to defend, when scrutinized. Why are there stricter requirements for seafarers serving on ships bigger than 500 GRT[8] than on ships smaller than 500 GRT in the CIE 143-2001[9]? The smaller ships usually, at least more often, are in near coastal traffic, perhaps also in littoral waters. They struggle with navigation lights ashore and on other vessels. The waters are busier with other small boats on crossing courses. They depend on visual navigation and perception of beacon lights, lighthouses and crossing traffic in challenging waters. On the contrary, bigger ships spend most of the time at the high seas, run on autopilot systems and with no other ship in the close vicinity. Sea pilots and tugboats assist them during port calls. - It is difficult to establish a logic rationale behind the decision of the differential treatment in the CIE 143-2001, at least based on evidence.
What is the correct cut-off point for visual acuity? It was set arbitrarily, as a compromise between the three parties participating in the development of the guidelines. The revised requirements in the STCW Convention in the Manila amendments[10] were more lenient for visual acuity than the old ones, but how did they arrive to this conclusion? Again – expert consensus and political arbitration. In the end, it will be a political decision at which distance, under which light and weather conditions, a seafarer should be able to notice a shipwrecked person, debris in the water, a ship’s lanterns or rock awash. Snellen’s decimal notation requirement of 0.5 was not set based on studies demonstrating the evidence or necessity for this cut-off point.
What about testing methods used in the medical examinations? Have they been validated for the purpose? Are they objective and can another examiner reproduce them? What should be the correct cut-off points for the decision of issuing a medical certificate to someone who will also have a duty as firefighter and use a breathing device?
It seems to me that we have a long way to go, until we are able to demonstrate the ‘necessary’ cut-off point for a given position or given on-board job task. Similarly, we have a long way ahead of us until we have the validated tools we need for the assessment.
Until then – we have to use what we have: International minimum requirements, based on low evidence expert consensus.
Most medical fitness standards and criteria for occupations in other industries are national or regional, sea pilots, car drivers, and rail engine drivers. Air pilots are assessed on regional requirements based on the Convention on International Civil Aviation[11]. Together with these, the international requirements for seafarers are the only medical fitness standards that are truly international.
Evidence as a basis for the medical examiner’s daily work
Relevant cut-off points are lacking in published scientific articles considering tests used for screening for working ability. The approved doctor faces quite a challenge when trying to substantiate a decision regarding the level of risk connected to the seafarer’s health condition. The heuristic approach still is the most important.
The medical examiner is supposed to assess vision, hearing, physical and mental function, use of medicines, and the risk connected to a known medical condition, sequelae from trauma or other disabilities.
The lack of evidence regarding vision requirements is challenging on a systemic and developmental level. It is, however, easy to carry out the necessary examination of a seafarer’s vision and assess the visual acuity against the established standards and criteria. The same goes – in principle – for hearing.
Physical fitness testing is more challenging. The criteria for assessment are those recommended in the STCW Convention Part B, Table B-I/9[12]. These requirements are general in their form, describing the tasks the seafarer is supposed to carry out, the corresponding physical ability, and that the doctor should check this ability. Which tests to use, and how to conclude with “pass” or “fail” still lack detailed guidance. The evaluation is left to the doctor’s own subjective assessment, based on his experience, knowledge of work on board and knowledge of the seafarer’s condition.
The challenges are even bigger when it comes to assessment of mental fitness. No psychometric or psychological tests have so far been validated for the pre-employment testing of seafarers[13]. This does neither seem to restrain the eagerness of many developers of medical fitness criteria for seafarers to require such tests, nor medical examiners to carry them out. Nobody knows if the individuals put ashore due to failing such tests actually would not be able to serve on board, and nobody knows if the individuals passing those tests actually are fit for service. A search in PubMed, March 2019, shows a glaring emptiness regarding publications on the issue. One historical survey article by Jones and Wessely from 2003 concludes that in selection of military personnel no instrument has been identified which can accurately assess psychological vulnerability[14]. The attempts have failed, because of false-positives, false-negatives and reluctance in the target population because of stigma[15].
The IMO/ILO guidelines use the ICD-10[16] classification for medical conditions. The criteria for assessment are sometimes difficult to understand, leaving a lot to the doctor’s own discretion.
The medical examiner is supposed to give an opinion regarding the likelihood for something to happen in a period of 2 years from the date of the medical examination. The international guidelines do not, however, give guidance regarding how big a risk should be for a ‘fail’ conclusion, or what may be allowed for a ‘pass’ conclusion. It is difficult to know the likelihood for a single individual to have a recurrence, a fit, a relapse, i.e. a medical incident in the future, more so during this limited period of two years.
By searching in review databases, one sometimes can find a likelihood for different medical incidents for the group of diagnoses relevant to the seafarer. Even though this is not equal to the individual likelihood for the particular seafarer to experience an incident in the next two years’ time, it will give us an indication for further consideration. A medical record, a medical examination, supplemental evidence from hospital reports and specialist opinions are valuable supplements that form the basis for the doctor’s final decision.
From heuristics to evidence-based decision-making
Will we be able – in the future – to base our assessment on evidence? Will we be able to document the necessity of taking a specific decision through a justification based on scientific medical knowledge? In the absence of certainty, probability is the best assessment tool. The probabilistic nature of medical selection is obvious. However, is it possible to improve the accuracy of the decisions?
Today’s medical selection of seafarers is not evidence based beyond the lowest level (expert consensus).
There are many different PEME[17] schemes for seafarers, international from the UN agencies IMO and ILO, and national from the many of the more than 170 flag nations[18], usually in compliance with the international guidelines from ILO and IMO. Some guidance is given from the EU regarding medical standards, issue and registration of certificates[19][20] and mutual recognition of seafarers’ certificates issued by member states. The different P&I Clubs[21], a number of manning agencies, ship managers and ship operators, require so-called ‘enhanced PEME’ schemes[22]. They have in common that they restrict employment opportunities more often than the IMO/ILO guidelines. They probably have a weaker evidence basis than the IMO/ILO guidelines, insofar as their group of experts are smaller, often self-appointed, and these schemes sometime give little or no guidance regarding interpretation of results, often relying on a number of laboratory tests[23], which are designed for diagnostic and therapeutic purposes, not for fitness assessment. One has to bear in mind that enhanced PEME schemes have an objective of loss prevention. This is not an objective of the statutory medical criteria. It is difficult to evaluate the enhanced PEME schemes in detail, as the criteria used for most of them are not publicly available.
From 2012, the Appellate Body of the Norwegian Maritime Authority introduced a structured approach to risk assessment in medical selection[24]. We will present the model later in this chapter.
[2] Oxford Centre for Evidence-based Medicine – Levels of Evidence (March 2009)
[3] Burns P B, Rohrich R J, Chung K C. The Levels of Evidence and their role in Evidence-Based Medicine. Plast Reconstr Surg. 2011 Jul; 128 (1): 305-310. PMCID: PMC3124652. NIHMSID: NIHMS288127. PMID: 21701348.
[4] Joint ILO/IMO Working Group on Medical Fitness Examinations of Seafarers and Ships’ Medicine Chest
[5] Report Joint ILO–IMO Working Group on Medical Fitness Examinations of Seafarers and Ships’ Medicine Chests. ILO/IMO/WGMG/2017/5/3 Appendix I.
[6] STCW Code Part A, Table A-I/9 with reference to CIE 143-2001.
[7] International Recommendations for Colour Vision Requirements for Transport. CIE 143-2001. ISBN 978 3 901906 09 1
[8] GRT: Gross register tonnage, a ship's total internal volume expressed in "register tons", each of which is equal to 100 cubic feet (2.83 m3)
[9] CIE 143-2001 International Recommendations for Colour Vision Requirements for Transport. ISBN:
[11] Convention on International Civil Aviation (Chicago Convention), Annex 1, Chapter 6 Medical standards.
[12] STCW Convention, Part B, Section B-I/9, Table B-I/9.
[13] Guidelines on the medical examination of seafarers, Part 3, XII, (xi), page 19. ISBN 978-92-2-127462-9 (print)
ISBN 978-92-2-127463-6 (web pdf)
[14] Jones E, Wessely S. Screening for vulnerability to psychological disorders in the military: An historical survey. Journ Med Screen 10(1):40-6 February 2003. DOI: 10.1258/096914103321610798.
[15] Jones E, Hyams KC, Wessely S. Screening for vulnerability to psychological disorders in the military: an historical survey. J Med Screen 2003;10:40-46
[16] The International Statistical Classification of Diseases and Related Health Problems (ICD), by the WHO
[19] Directive 2008/106/EC of 19 November 2008 on the minimum level of training of seafarers
[20] Directive 2005/45/EC OF THE EUROPEAN PARLIAMENT AND OF THE COUNCIL of 7 September 2005 on the mutual recognition of seafarers' certificates issued by the Member States and amending Directive 2001/25/EC
[22] Basurko O F. The role of manning agencies or the seafarer’s recruitment in the maritime employment market. HAL id: hal-01470405.
[23] Horneland AM, Stannard SL. Decision aid for the use of additional tests during the pre-employment medical examination (PEME) of seafarers. Int Marit Health. 2017;68(2):90-98. doi: 10.5603/IMH.2017.0017. PMID 28660611.
[24] GUIDANCE TO REGULATIONS ON THE MEDICAL EXAMINATION OF EMPLOYEES ON NORWEGIAN SHIPS AND MOBILE OFFSHORE UNITS
C.8.2 Development of standards
Details
ALF MAGNE HORNELAND
The probably oldest trace of statutory medical standards for seafarers in Norwegian seafaring history can be found in “Magnus Lagabøtes Landslov”[1] (AD 1276) where it was required that men capable of standing a beacon watch are those with healthy eyes, ears, feet, men that are free and of age, able for military service, domiciled and not a foreigner[2].
Requirements for sailors’ ability to work, to see and to hear, came earlier in the military navies than in the merchant navy. Already during the 17th century, one can find traces of such requirements in naval history[3].
In the late 1800s, the Norwegian maritime authority became concerned about merchant seafarers’ health condition[4]. They did not issue requirements for pre-employment medical examinations at this time, but focused on first aid, equipment for treatment of illnesses and dietary requirements.
Norway introduced mandatory pre-employment medical examinations from 1903[5], probably among the earliest requirements for any merchant navy. The requirements were simple: There were demands regarding visual acuity and colour vision, and the seafarer should provide a declaration that he did not present symptoms of malignancy and contagious diseases, including contagious tuberculosis[6].
Development by the UN Agencies
During the 20th century, several steps were taken regarding improvement of the regulations on medical examinations. The international process of development was initiated by the ILO shortly after its establishment in 1919[7], with the “Medical Examination of Young Persons (Sea) Convention, 1921 (No. 16), followed by the “Medical Examination (Seafarers) Convention, 1946 (No. 73). These instruments are now incorporated in the Maritime Labour Convention, 2006 (MLC, 2006).
The present Norwegian regulations from 2014 are based on the International Guidelines on the medical examination of seafarers of 2013 from ILO[8] and IMO[9], and the fitness criteria are identical to those of the International Guidelines.
After the International Maritime Organisation was established in 1958, the organisation started to develop qualification requirements. The qualification requirements also included health requirements in the STCW Convention, 1978, with later amendments. These standards focused on eyesight and hearing, as well as recommendations for physical fitness, although not specified in much detail.
Attempts to harmonize the requirements resulted firstly in the Guidelines for conducting Pre-sea and Periodic Medical Fitness Examinations for Seafarers[10] published jointly by the WHO[11] and the ILO. It was, however, not until 2013, that ILO and IMO jointly issued the “Guidelines on the Medical Examination of Seafarers”[12], based on MLC 2006[13] and the STCW Convention[14].
These guidelines have been used by some countries as minimum requirements in the development of national regulations, by other nations directly as they are, without further alteration.
The focus has gradually shifted from being solely concerned about working ability, avoidance of threats to ship operations and other crewmembers, to also including the aspects of advice on medical care and prevention of illness of the seafarer.
Regional development: the EU
In parallel to the work in the UN agencies, national and regional authorities started similar processes. The EU introduced statutory standards for medical fitness examination from 31 December 1995[15], based on the qualification requirements of the STCW Convention[16]. The regulations were more of a formal character, making medical fitness a legal requirement of the EU, albeit referring to the requirements of the ‘administration’ (national requirements of a member state). The present legal framework in the EU is the Directive 2008/106/EC[17], still not describing detailed standards, rather referring to member states requirements.
Development in seafaring countries
Seafaring countries are, almost without exception, members of the IMO and ILO. Membership responsibilities include implementation of the medical fitness requirements of the MLC 2006 and STCW conventions and, as a consequence, adoption of the International guidelines on medical examination of seafarers. The interpretation of these conventions and guidelines varies somewhat between member states regarding training of approved doctors and quality assurance systems. Some countries refer directly to the international guidelines as mandatory without making national arrangements; others develop complicated systems with national details, guidance and training for doctors, quality systems[18], and measures to prevent forgery of medical certificates[19].
Some countries have approved doctors outside their own borders, e.g. the UK, the Netherlands, Germany and Norway. Other countries rely on the national certificate of the seafarer’s home country.
The P&I insurers[21] (see Ch. 3.8 and 5.13) had rising concerns regarding the health of seafarers in major manning countries during the last decade of the 20th century[22]. Several of the P&I Clubs carried out projects regarding loss prevention by means of more detailed and so-called ‘enhanced’ programmes for medical examination. Today most P&I Clubs implement such programmes[23].
Contrary to some statutory programmes that require laboratory tests on indication only, the majority of these enhanced PEME programmes include a list of mandatory laboratory tests. Such laboratory tests when used in hospitals or general practices are developed for diagnostic purposes in a clinical setting where there is an indication and a certain pre-test probability. Such tests are not designed for screening a healthy population for possible medical conditions. Despite of this fact, some enhanced medical schemes include many of those tests as mandatory. (See later for a more detailed discussion on the use of such tests.)
In addition to sharing the concerns about safety for ship, crew and the seafarer, the enhanced programmes also include objectives like loss prevention and regularity of operations. As can be expected, they are not congruent with the statutory schemes.
[1] Magnus Lagabøte (Magnus the Lawmender, or Magnus Haakonsson or Magnus VI of Norway) promulgated the national law, “Magnus Lagabøtes Landslov”, a unified code of laws to apply for the whole country, including the Faroe Islands and Shetland.
[12] ILO/IMO: Guidelines on the medical examination of seafarers; Preface. ISBN: 978-92-2-125097-5 (Web pdf)
[13] Maritime Labour Convention 2006 (MLC 2006) (ILO)
[14] International convention on Standards of Training, Certification and Watchkeeping for Seafarers, 1978 as amended (IMO)
[15] Council Directive 94/58/EC of 22 November 1994 on the minimum level of training of seafarers
[16] International Convention on Training, Certification and Watchkeeping for seafarers 1978, 1995 revision (IMO)
[17] DIRECTIVE 2008/106/EC OF THE EUROPEAN PARLIAMENT AND OF THE COUNCIL of 19 November 2008 on the minimum level of training of seafarers (recast)
[18] Quality system for seafarers’ doctors. Circular series V. RSV 12-2014 of 22/10/2014. Norwegian Maritime Authority
[19] New Regulations on the medical examination of employees on Norwegian Ships and mobile offshore unites. Circular – Series R. RSR 02-2014 of 05/06/2014. Norwegian Maritime Authority.
[20] PEME = Pre-Employment Medical Examination. The term is used to describe the mandatory medical examination prior to being employed for work, or periodically during employment for work.
[21] Protection and indemnity insurance or «P&I insurance» is a form of mutual maritime insurance, provided by a P&I Club covering loss of life and personal injury to crew, passengers and others on board, cargo loss and damage, pollution by oil and other hazardous substances, wreck removal, collision and damage to property. P&I insurance is different from “marine insurance” (H&M – hull and machinery) offering cover for shipowners and cargo owners. The International Group of P&I Clubs website: https://www.igpandi.org/about accessed 2019-04-23
[22] Gard Enhanced PEME programme for Filipino Seafarers is expanding, 2016-07-13. Gard Website.
[23] Gard’s pre-employment medical examination scheme. Insight 178, 2005, 01. May 2005.