Working on board has its own occupational risks with variations due to the nature of the work and the type of vessel. Care of the injured or ill seafarer is usually the responsibility of a deck officer, often the first officer, but ultimately the ship’s Master has final responsibility.
The officer responsible for medical care on board may handle many minor injuries and ailments. He should keep good records of all consultations and this is discussed further in Ch 2.8. He may seek advice from a TeleMedical Assistance Service (TMAS) as there are limits to the capabilities of ships’ officers to diagnose and treat. Improvements in technology and communications make obtaining TMAS advice easier. (Ch. 5.7). In addition, the limitations of equipment and medicines on board, together with the medical experience and training of the officers, influence care provided (Ch. 5.3). Publications such as the International Medical Guide for Ships[1] or a national equivalent cover the practical treatment of such cases and this is beyond the scope of this text.
Minor injuries
The nature of the work on board may result in minor injuries due to, for example, slips, trips and falls, falling or swinging objects, chemical incidents, and manual handling. Burns are more likely to occur in the engine room or galley environments. The types of minor injuries seen may be lacerations, bruising, sprains and strains, burns including sunburn, head injury, eye injuries or simple fractures. Improvements in risk assessment of on board procedures, and the correct use of safety equipment, should reduce the number of minor injuries sustained. Please see Ch. 6.2 for additional information on risk assessment.
All those working at sea will have rudimentary knowledge of first aid to enable them to initially treat injuries and get help. Mandatory training in first aid is focused on lifesaving techniques rather than, for example, simple wound cleaning and dressing. Even the more advanced medical care training is limited to immediate actions rather than long-term care, for example, the assessment of wounds and ongoing management. The availability and choice of wound dressings is limited in the mandatory equipment to be carried on board and additional equipment carried by choice will vary. (Ch. 5.5). Simple supplies and medicines readily available ashore for managing small wounds, insect bites, and superficial burns, may not routinely be kept on board. Provision of these items should be considered and based on the type of injuries sustained on board a vessel. This will make the management of minor injuries easier to fulfil.
Minor illness
The clinical knowledge of the officer dealing with the patient may be very limited as will the accuracy of monitoring the patient’s observations and clinical signs. Without the assistance of TMAS, symptoms may not be recognised, incorrect diagnosis made and inappropriate treatment given.
Minor illness may not even be notified to the officer responsible for medical care on board and may be self-managed. Reasons for this will vary but it is important that all illness is reported in case the situation worsens and becomes an emergency to be dealt with. In particular, some early signs and symptoms may indicate a higher risk of serious underlying problems for example, any decline in consciousness after a bang on the head, or a raised temperature with signs such as photophobia, stiff neck or headache.
Major illness and Injury
Major illness may develop slowly or be sudden in nature. Medical advice should always be sought from TMAS, as the officer responsible for dealing with the problem with not have sufficient knowledge to manage the situation appropriately. Misdiagnosis, or delay in treatment, may have serious consequences for the sick crewmember. Any delay in getting advice from TMAS may also affect how quickly evacuation from the ship may be achieved.
When serious injury occurs rapid first aid will be required. As with major illness, help should be sought as soon as possible, but there should be no delay in applying first aid to the casualty.
[1] International Medical Guide for Ships. ISBN-13: 978-9241547208 ISBN-10: 9241547200
D.7 Telemedical assistance services
Details
ELIAS VAN HAVAERBEKE; ARNE JOHAN ULVEN – FROM 2ND EDITION.
Introduction
Telemedical maritime assistance services (TMAS) are remote medical advice services designed to provide medical assistance to seafarers and others on a ship. Quick and easy access to such a service is a key element of medical care on board and these services are primarily used by seafarers on board ships without a physician. Ship’s doctors or other health care professionals may also seek assistance when necessary. The service may be organized and sponsored by member states of the International Maritime Organisation (IMO), or may be a private enterprise. Legally, every member state of the IMO is obliged to provide a TMAS at all times, to all ships and free of charge. The Master or the officer responsible for medical care on board a ship should request remote medical advice from a TMAS centre, as and when they consider it necessary. It should be noted that TMAS provides an advisory service and that the final decision and responsibility for the treatment of the patient, including evacuation or diversion etc. is always for the Captain on board.
TMAS forms an integral part of the Search and Rescue (SAR) capability of many nations. Medical evacuation of the patient can be required and in this case, a Maritime Rescue Coordination Centre (MRCC) or Joint Rescue Coordination Centre (JRCC) can assist in organising this evacuation if available. Good cooperation between TMAS centres and MRCC/JRCC is key for this kind of operation. More information on Search and Rescue is available in Ch. 5.8.
Regulation of TMAS
TMAS is regulated by a convention that is the product of the cooperation between the IMO and the International Labour Organisation, convention 164 of ILO Health Protection and Medical Care (Seafarers) Convention[1]. As TMAS is seen as integral part of SAR, additional requirements are set in the IAMSAR (International Aviation and Maritime Search and Rescue) manual[2].
The Maritime Labour Convention 2006 (MLC)[3] also makes reference to TMAS and states that ‘the competent authority shall ensure by a prearranged system that medical advice by radio or satellite communication to ships at sea, including specialist advice, is available 24 hours a day; medical advice, including the onward transmission of medical messages by radio or satellite communication between a ship and those ashore giving the advice, shall be available free of charge to all ships’.
Differences in provision around the world
Despite the regulations, the provision of TMAS varies hugely around the world with significant differences in the availability, capability, range of services and quality. In Europe, almost every country provides remote medical assistance through a TMAS centre. In other parts of the world far less countries meet the obligation of establishing a TMAS centre. For example, India, a country with approximately 13% of all officers at sea, does not offer this service.
TMAS providers differ in some aspects, such as whether they are part of a hospital organisation or if the center is manned 24/7 by dedicated doctors. Some countries choose to provide the bare minimum whilst for others, no effort is too much to create a professional organization. Some services only offer advice and guidance if the case needs to be evacuated from a vessel whilst others offer ongoing medical advice for any concern.
In Denmark, there is an exception to the rule that the Master remains responsible for the ongoing care of the seafarer. Upon calling the Danish TMAS centre and agreeing that a sick or injured seafarer should be evacuated, the medical responsibility is transferred to the treating physician.
Private vs state providers of RMA
TMAS can be a governmental service funded by the state, or a private service. Private providers are often, but not always, a regular doctor doing a consultation over a certain distance from shore. Large assistance companies with 24/7 manned operation platforms may also offer telemedical assistance to ships around the world.
There are two key differences between private and public providers of TMAS:
Public providers organized by the state work within the IMO-set legal frame for TMAS centres. Private providers do not have to follow any rules or guidelines set by the IMO.
State run providers are supported financially by the flag state whereas the state does not support private providers in any way.
For survival, a private organization needs consultations and the shipping company must usually pay for access to the service. Payments may be annual or per consultation. It is vital for a private organization to provide a quality service, otherwise companies will take their business elsewhere. A state organized and funded TMAS service does not have this need for a minimum number of consultations because the income is guaranteed by the state. Therefore, both systems have a different way to guarantee the quality of the service provided; state run facilities because they follow a minimum set of requirements set by the IMO and private providers simply because they still exist and retain clients.
There is an increasing desire to improve cooperation between TMAS services to ensure quality and consistency in the service. Closer cooperation would also offer improved information about the diagnoses etc. of cases that are handled on board.
Communication
Communication is key for a quality and efficient TMAS. It may be spoken or written and pictures and videos can be sent to clarify certain symptoms. Establishing this communication is possible by multiple available means including VHF, HF, MF (satellite) telephone, e-mail and INMARSAT.
The List of Radio determination and Special Service Stations contains contact details for the state organized TMAS services. This list is on board and available in the ALRS Vol I. For most of the TMAS-centers, communication channels mean all possible modern ways of communication: via (satellite) telephone, INMARSAT, e-mail, VHF, HF and MF. A TMAS service can also be reached by contacting a MRCC/JRCC.
Some TMAS services work in a different way. For example, only one or limited ways of communication can be used. In Portugal for example, the only way to establish contact is by using VHF channel 16. Another possibility is that a TMAS service can only be contacted by first contacting an MRCC/JRCC or another organization such as the coast guard.
Ship’s officers generally use their own language when they contact their national TMAS. For all other communication and to other centres, English is generally used. Every medical consultation must be recorded in accordance with the national regulations of each TMAS centre.
Written communication
Communication with ships in morse code on long and medium waves became possible from 1906. The coverage was mostly near coast areas until after World War II when short wave was also used and the coverage became worldwide. Despite its superior efficacy, the use of morse code decreased during the late 20th century. It was finally replaced completely by the Global Maritime Distress and Safety System (GMDSS) on February 1st 1999. Now clear text could be transmitted without the need for interpretation, the predecessor of today’s email. However, the advent of the internet in the 1980s made telex obsolete and the telex networks closed down around 2000. The satellite era and the advent of the internet allowed for the development of the e-mail system that is the predominant mode of written communication ship/shore today.
The advantage of written communication is that the communication is well documented and any language issues or misunderstandings may be reduced. The disadvantage is the slowness of the process. Pictures, video and vital data can also be transferred and add great value when appropriate.
Voice communication
Radio communication with ships today is rapidly declining except for VHF in coastal regions. Telephone communication via satellite is by far the most used mode for long distance communication in the shipping industry. The signals pass from the land-based telephone net, or mobile net, via an earth station and a satellite to the recipient, and back. The audio is usually of a high quality, even if some echo or delay may occur.
The important advantage of voice communication is the speed of information exchange. When immediate aid is necessary, written communication can be far too slow. Voice communication can be supplemented with written communication as necessary. Documentation of voice communication is possible by means of voice logs. In addition, other important aspects of medical consultations, such as reassurance, are easier to deliver by voice. However, voice communication is not without pitfalls, the most important being language problems. Some ship’s officers do not have the necessary knowledge of English and this can cause huge issues in establishing the medical problem, its severity and advising on appropriate care and action. Some nations have online interpretation services for civil purposes. The establishment of an international service of this kind would be a natural task for the future cooperation among TMAS services.
Standards of communication
Both the TMAS doctor and the ship’s officer should have an appropriate level of English and the TMAS doctor should be careful to use plain language and refrain from professional jargon.
The use of standard forms may also improve communication and these can be found on the International Medical Guide for Ships 2007[4]. Officers would benefit from consulting these forms before calling the TMAS service and TMAS doctors should be familiar with them.
Difficulties in communication
In practice, the English vocabulary of many seafarers is not good enough to communicate about medical problems. In addition:
Medicine is not practiced the same around the world. The trust of the officer responsible for medical care and the TMAS doctor is a critical factor.
Different cultures have different ways of communication. Non-explicit links can be even easier lost in the communication. The communication is already of a basic form with many obstacles between the doctor and the patient.
The TMAS physician
Although the conventions stipulate that doctors who give tele medical advice to ships shall receive proper training and be aware of shipboard conditions, ‘proper training’ is not defined in any detail. It seems fair to suggest that the advising doctor should have appropriate knowledge of
Spoken and written English
Ship types and positions on board
Dangerous cargoes and their potential health effects
Medical facilities around the world and the variation in services and quality
The variations in the content of medicine chests on different vessels
The variations in medical knowledge, training and skills on board a ship
The variation and limitations in the ship’s medical centre
The role of Maritime Rescue Coordination Centres (MRCC) and Joint Rescue Coordination Centres (JRCC) and SAR services
The implications of culture, hierarchy on board, economy and possible consequences of getting ill or injured for further employment of the seafarer
The options and risks of medical evacuation
TMAS in the offshore industry
The operators in the international oil industry will normally be obliged to arrange and finance their own TMAS and SAR services due to national regulations. Ships serving the offshore installations will normally not be included in this service and will have to contact the regular TMAS services unless they are within a very short distance from the installation, as defined by the operator.
[4] International Medical Guide for Ships. 3rd edition. Geneva: World Health Organisation. 2008
D.9 Evacuation of the sick or injured seafarer
Details
SUE STANNARD
Introduction
Although the evacuation of a seafarer or passenger from a ship is not a common occurrence on many vessels, it does occur. In 2017, Radio Medico Norway treated 1316 patients, of which 15% or 200 were evacuated.
Evacuation options include:
evacuation of the patient at the next port. This can either be the next port of call in the normal trading pattern of the vessel or the nearest appropriate port involving diversion of a ship from its planned route.
ship-to-ship evacuation, for example the patient can be transferred to a ship with a doctor or other health care professional on board or onto a fast rescue craft or other vessel heading to shore. This depends on the presence of such a ship in the vicinity and appropriate weather conditions.
ship-helicopter evacuation. This relies on many factors, included but not limited to weather, availability of a helicopter, the range of the helicopter and position of the ship, see below.
Every evacuation, whether ship-to-shore, ship-to-ship or ship-to-helicopter is associated with complications related to physical movement from bed to stretcher and from one place to another. These may range in severity from the pulling out of intravenous lines or dislocation of immobilization splints to life-threatening ones such as the pulling out of endotracheal tubes or accidents involving the entire stretcher and patient during the transfer. There are well documented incidents of more harm done to the patient in transfer than in staying where they were[1].
Risk assessment
Whether or not to evacuate and if so, the appropriate method of evacuation depends on multiple factors and must be determined on a case by case basis. These factors include the following.
Medical factors
These should be the primary factors in the risk assessment but they cannot be taken in isolation. In general, the reasons to initiate the evacuation of a patient from a sea-going vessel are:
Serious injury or illness that may cause invalidity or death and that requires care that cannot be given on board before the scheduled arrival in the next port of call. The risk of potential invalidity needs careful assessment. For example, the decision whether and by which mode a patient is evacuated may differ depending whether a critically injured finger is the fifth or the second one, and whether it is on the patient’s dominant hand.
The need for further investigation that cannot be performed on board and that cannot wait until the next port of call and the results of which would change the management of the patient, for example, radiology investigations.
Management of a seafarer with an infectious disease who cannot be appropriately isolated on board and whose ongoing presence on board may infect others and threaten the safety of the ship. If the patient is suspected of having a disease that may come under the International Health Regulation, 2005 for communicable diseases, it is essential for the TMAS doctor to notify all parties concerned, namely the respective MRCC/JRCC and the evacuation organization. The Master, under these circumstances, is under a legal obligation to notify the Port Authorities of the next port of call using the Maritime Declaration of Health. More information on the International Health Regulations is available in Vol VIII.
Other factors to consider include but are not limited to:
Clinical condition of the patient. The old saying of ‘never move an unstable patient’ should not be dismissed. However, this must be taken alongside consideration of what medical care can be given on board and what medical care is necessary. Is the patient as well and stable as they can be given the limitations of care and their surroundings?
Need for care in transfer. What care is necessary in transfer and can this be delivered must be considered. The care required in transfer will depend upon a number of factors including the medical condition of the patient, the length of transfer or time to port if the ship is diverted, the number and experience of staff accompanying the patient and what equipment will be available. If appropriate care cannot be delivered is this the best option?
The time window for receiving specialist investigation and treatment in order to improve the outcome for the patient must also be considered. For example, thrombolysis after a cerebrovascular incident must occur within a certain time after the onset of symptoms for the benefit to be worth the risk.
Fitness to fly. Although less of a consideration in helicopter flights than fixed wing aircraft due to the lower altitude of flight, the potential effects of changes in air pressure on the volume of entrapped gasses in the body and a relative lack of oxygen in the unpressurised helicopter should be taken into account.
Psychiatric patients may become uncooperative or even violent during the evacuation process. This can be particularly dangerous at the point of transfer or in the confined space of a helicopter. Appropriate personnel may be necessary to use restraint or medication as required.
Economic factors
These may be of particular interest to the Master who may feel under pressure to keep any costs to be incurred and disruption to the ship’s operation as low as possible. Factors include but are not limited to the cost of:
the evacuation itself e.g. the helicopter or rescue craft with personnel,
land transportation and any medical expenses in the proposed destination, These aspects will be cost free in some countries but may incur very large costs in others
port agent fees for assistance provided
additional fuel for any diversion or increase in speed to reach port or another vessel more quickly
additional berthing for the ship if a route/itinerary is changed and additional time in port or time at anchor in port limits is required
disruption to the ship’s operation eg fishing itineraries and length of voyage, loading or unloading cargo with the hire of extra gangs in port, port calls and tours for passengers
Geographical factors
These are often beyond the control of those making the decision and factors include but are not limited to:
distance to shore. This will not only affect the timeframe in which an evacuation can be done but also how it is done. Other ships may be limited by distance and cost and helicopters have a fixed range depending on their type.
weather conditions form a large part of the risk assessment in many cases. Certain weather conditions make helicopter evacuation or the transfer of a patient from one ship to another very difficult if not impossible. The decision as to whether or not to proceed with the evacuation in these conditions will depend on many factors such as the experience of the flight crew, wind direction, visibility, wave height etc.
distance to appropriate medical care. It may not be appropriate to reach the nearest land as the required medical care may not be available there, but only further along the coast. Any planning of an evacuation must include the actual destination of the seafarer, be that a medical facility or an airstrip for ongoing movement.
Practical factors
Appropriate planning may be able to reduce these factors, including but not limited to:
availability of other necessary assets e.g. ground ambulance to move the patient from where they are landed ashore to the medical facility
the availability of the necessary assets e.g. a helicopter. The number and location of appropriate craft varies hugely around the world’s coastlines.
Motion sickness. This can affect anybody on any ship but may be exacerbated in sick or injured seafarer, and any accompanying person, when on board a small, fast craft or in a helicopter. The act of vomiting may have a serious impact on the seafarer’s medical condition and consideration should be given to the use of anti sickness medication on the advice of the TMAS doctor.
Risks to ship and others on board. Helicopter evacuations place the ship, the helicopter and all on board at risk should the helicopter crash and land on the ship. Increasing the speed of a vessel may make others unwell with motion sickness and increase the risk of injuries on board.
Risk management
Many of the factors mentioned are unique to each case and in many specific instances, they are beyond the control of those involved in making the decisions. However, certain steps may be taken to ensure that the likelihood of an evacuation and an associated risk occurring is reduced or, should it occur, the impact is minimised. Further information on risk management is available in Ch 2.5.
Steps in the risk management of medical evacuations may include:
Appropriate medical selection of seafarers – the right seafarer for the right role on the right ship. Further information on the medical selection of seafarers is available in Ch 4.8.
Appropriate training of medical officers in medical care. A ship owner or ship manager must ensure that seafarers have appropriate certificates of competency, including medical care as outlined in STCW. More information on the training of seafarers in medical care is available in Ch 5.3.
Appropriate medical chest on board, suitably stored and checked as required. More information on the medical chest is available in Ch 5.4.
Appropriate medical guide on board in an easily accessible place. This is included in the MLC 2006[2]
The use of Medical Emergency Response Plans outlining an appropriate TMAS, MRCC/JRCC, evacuation resources, shore based medical care etc. It may be very difficult if not impossible for this to be done for ships on worldwide trading routes but for other ships on routes that are more regular or limited in location it should be considered. The use of a Medical Emergency Plan could be incorporated into the voyage plan whatever the itinerary.
The inclusion of relevant policies and procedures as part of the ship’s safety management system to include communication with TMAS and other shore based organisation, documentation required for the evacuation of a seafarer or passenger, transfer of the patient on board the ship, helicopter operations, ship to ship transfer etc. Advice in these areas is available from many sources e.g. the International Chamber of Shipping Guide to Helicopter/Ship Operations[3]
Regular training on board of crew in the practical aspects of the above policies and procedures.
Options for evacuation
Ship-shore
If the medical situation of the patient allows and the distance towards a suitable shore-based medical facility is within acceptable reach in distance and time, the safest and most comfortable mode of evacuation is often by the vessel itself delivering the patient. This may imply that the vessel changes its course/ itinerary towards a nearer port than the one that was scheduled. Arrangements will need to be made for appropriate land transportation to meet the ship and for appropriate receiving care for the seafarer. The TMAS doctor, the vessel’s shipping agent or MRCC/JRCC may be able to assist in this.
Ship-ship
It may be the most appropriate option to arrange to meet with another vessel and transfer the patient. This may have two different motives.
More rapid and easier transfer of the patient to shore. This may involve the use of a pilot boat, coast guard vessel, fast rescue craft from a cruise ship or other vessel, another vessel heading at greater speed for port, eg another fishing vessel. Some of these options will also provide an additional level of medical care that can be used to stabilise and continue care for the patient during transfer.
Improved level of care. Sometimes the patient may be transported to a vessel offering more advanced medical care. Naval vessels, passenger cruise vessels and hospital ships are some examples of ships that will offer help in case of medical emergencies, sometimes far out at sea.
The risks of transferring a patient from one vessel onto another at sea must not be underestimated. Even if the sea is calm, walking down the gangway for a sick or injured person, and stepping onto a smaller vessel always has its potential hazards, regardless of the willing help offered from all sides. If the patient needs to be transported on a stretcher, this stretcher will need to be lowered by ropes down the side of the vessel, or via side doors if they are available, to be landed on the deck of the smaller craft below. In cargo ships the deck may be as high as 12 metres above the level of the sea.
Two large vessels adjoining at sea may sometimes be unfeasible. Transfers at sea onto larger ships as mentioned earlier may require an intermediate transfer in one of the vessel’s dinghies, thus implying two transfers ship-to-ship.
Ship-helicopter
Helicopters are a swift and efficient means of transporting the patient towards more advanced medical help. A helicopter’s range, however, is limited to an average of 150-200 nautical miles outside the coast, this being primarily a question of fuel supply. Newer craft are capable of increasing distances but there availability may well be restricted.
Helicopters involved in the evacuation of a seafarer from a ship maybe part of the national SAR capability, eg the Norwegian Coast Guard and the United States Coast Guard. These helicopters are manned with a doctor, intensive care nurse or medic who are well trained in medical emergency treatment and transportation. This implies that in getting help from a helicopter to evacuate the patient, expert medical personnel are also available offering a higher level of medical care, all be it in the relatively confined space of a helicopter. The helicopter and its crew will also bring in advanced medical equipment such as life-support and monitoring equipment and a defibrillator. However, in other areas of the world the helicopter and crew used may be a private provider with little or no experience of or training in maritime operations, no medical crew on board to offer care to the patient in transfer and no additional equipment. They are simply a means of transportation. In other areas there may be no helicopter evacuation capability at all, or a very limited number of craft serving a large geographical area.
Decision to evacuate
The Master, the officer responsible for medical care or the TMAS doctor, may identify the potential need for evacuation. However, many others may become involved in the discussion including
staff from the nearest MRCC/JRCC, medical or other,
helicopter and other vessel crew assessing weather and sea conditions
doctors or others at the receiving facility
doctors or others from the port health authority
the ship owner or operator and/or their insurer
Ideally, the parties will agree on the decision to take but there may be differences of opinion with each party having a different point of view and differing priorities. In cases where differences of opinion arise, these arguments should be clearly brought forward, each respecting each other’s professional arguments and come to a common understanding whether an evacuation is necessary and according to a thorough risk assessment. It is important to ensure that medical confidentiality is maintained as far as possible in all discussions, particularly those involving non medical staff. Further information on ethics and confidentiality is available in Ch 2.9.
Preparing the patient for evacuation
It is important that all relevant information should be collected and accompany the patient, preferably in a plastic sealing or envelope. It is essential that these comprise:
the patient’s passport, seaman’s book, vaccination book
medical reports from the time on board that include as a minimum:
details of onset of illness or injury
description of medical findings and a log of the development of these in the course of lapsed time, especially concerning the vital signs such as heart rate, blood pressure, breathing frequency, temperature, conscious level etc.
therapeutic measures taken, especially which medication was administered, how and when
a copy of all correspondence with TMAS or with doctors in previous ports concerning the patient.
personal belongings, as the patient is unlikely to immediately return to the vessel. These should at least include some cash, bank cards and a mobile phone and charger. If practicable and time permitting, his suitcase and personal effects should be packed and sent along with him.
It may also be necessary to prepare accompanying family members in the case of a passenger and to contact the seafarer’s or passenger’s next of kin. Shore side personnel may do this but it is important to ensure that it is not forgotten. In addition, if they are not already involved, relevant personnel and organisations ashore, for example the receiving medical facility, should be contacted and updated with the plans, contact details for the seafarer and relevant company contacts. An agreement should be reached about follow up of the seafarer once ashore. More information on management of a landed seafarer ashore is available in Ch. 5.10 and 5.11.
Medical care around the world
Variation
Medical facilities vary hugely in different areas of the world. Variation can be seen in
The availability of specialty services such as neurosurgery, tertiary level intensive care and support services such as interventional radiology, range of laboratory investigations
The practice of medicine, protocols followed, procedures performed, medication used etc
The level of nursing care and what assistance is given by the nursing staff eg feeding, provision of food etc
The input and role of the patient’s family in providing basic care such as washing
The buildings and their state of repair
The availability of medicines and other equipment e.g. ventilators
What is available where?
To keep an accurate, up to date and comprehensive list of all the medical facilities around the world, even limited to the coastline is almost impossible. The amount of information gathering and the speed at which things change make this a huge challenge although some of the cruise companies have attempted it in the past. Information may be available:
TMAS or MRCC/JRCC services may have a good oversight of what is available in their own and surrounding nations.
Assistance companies have a documented list of providers in different areas of the world but this is limited to their operating area.
Shipping companies may have built up their own list of medical facilities in ports that they visit often,
Local port agents will be aware of some of the facilities locally. However, they are usually non-medical and may not be aware of what medical care is required as opposed to what can be provided. In addition, there is often a degree of local politics involved in making referrals.
The provision of medical care within a country may be variable depending on location and population. Not all ports, towns or even cities may have a full range of medical services depending on the level of health care nationally and how it is organised in country. Whilst MLC 2006 and other international regulations clearly state that a nation ‘shall ensure that seafarers on board ships in its territory who are in need of immediate medical care are given access to the Member’s medical facilities on shore’, health care that is not available for the local population cannot suddenly be available for a seafarer.
Care of the landed seafarer
Managing ongoing medical care may involve the
Guarantee of payment for or pre-payment of the hospital costs. It is advised that appropriately trained staff monitor the treatment and costs incurred, in order to ensure that care is appropriate and necessary.
Liaison with the seafarer, his employer/manning agent/insurer and next-of-kin while he is in hospital. Care must be taken to ensure medical confidentiality.
Practical support of the seafarer in terms of basic needs and to ensure communication etc to family and friends. He will also appreciate the provision of books, magazines etc, ideally in his native language, snacks and time to talk with another person that understands his position.
Arranging for repatriation home back home once the treatment in hospital is complete or a further evacuation for a higher standard of medical care if required.
Further information on this area is available in Ch 5.10 (Port Health care) and Ch.5.12 (Repatriation and Rehabilitation – may need to cross reference different sections).
Maritime search and rescue (SAR) refer to a wide range of medical and logistical measures that aim to prevent loss of health or life in the event of distress at sea.
The nature of SAR operations vary according to geographical and climatic constraints, as well as the availability of SAR assets. SAR operations may take the form a coordinated response, for example, led by a maritime rescue coordination centre (MRCC) and including land-based, airborne and floating assets. It may involve a single responder, for example, from another vessel in the proximity of the individual or unit in distress. Often it is somewhere in between. The ‘search’ of SAR is the effort to locate a person or vessel in distress and the ‘rescue’ includes the operations aimed at retrieving a person or a vessel in distress, providing medical and non-medical assistance and evacuating individuals in need to a place of safety.
Maritime search and rescue is regulated by the International Maritime Organisation (IMO) Convention on Search and Rescue (SAR convention)[1], the Maritime Labour Convention 2006[2] (MLC) and the United Nations Convention on the Law Of the Sea (UNCLOS)[3] and is the shared responsibility of all seafarers, as well as coastal states. Telemedicine is an integral part of maritime SAR as discussed in Ch. 5.7.
History of search and rescue
The dangers at sea have troubled seafarers and challenged seafaring for as long as man has navigated the seas. Throughout history, shipwrecks have claimed the lives of countless numbers of seafarers and illnesses, disease and malnutrition at sea have claimed the lives of many more.
It has been argued that the dangers faced at sea have promoted a sense of community and a shared understanding between seafarers, that they will come to each other’s assistance in the event of an emergency. In that sense, search and rescue is by no means a new invention.
The Rhodian Sea Laws provide the first written reference to the management of distress at sea. Recorded in 600-800 AD, the law detailed how the lightening of ships by dumping cargo in the event of maritime distress was permissible in the Byzantine empire, and how coming to someone’s rescue would be compensated. Although it should be noted that the primary concern of the law was the value of the cargo, rather than the lives of the seafarers, it may be considered an early precursor to modern day search and rescue at sea.
In the later mediaeval sea laws, including the French Rolls of Oleron in the 1200s and the Wisby Sea Law in the 1500s, a stronger emphasis on wellbeing of seafarers were included, introducing penalties for those harming or plundering a shipwrecked seafarer. Further information on the history of the maritime industry is available in Vol IV.
The modern day legal framework
The first legal obligation to come to a seafarer’s assistance was introduced with the Brussels Convention for the Unification of Certain Rules with Respect to Assistance and Salvage at Sea in 1910. This stated that ‘every master is bound, so far as he can do so without serious danger to his vessel, her crew and her passengers, to render assistance to everybody, even though an enemy, found at sea in danger of being lost’.
Later, in 1974, the Safety of Life at Sea (SOLAS)[4] convention called for the establishment of coastal maritime search and rescue (SAR) services and in 1979, the International Convention on Maritime Search and Rescue was agreed[5]. It states that ‘Every coastal State shall promote the establishment, operation and maintenance of an adequate and effective search and rescue service regarding safety on and over the sea and, where circumstances so require, by way of mutual regional arrangements co-operate with neighbouring States for this purpose.’
Later conventions, have included the United Nations Convention on the Law of the Sea (UNCLOS 1982) and the International Convention on Salvage of 1989[6], the latter replacing the Brussels Convention. These have reaffirmed the shipmaster's duty to render aid in the event of distress, which forms the basis of the modern day search and rescue legal framework.
What is distress at sea?
Distress at sea is a situation in which severe and imminent danger threatens a person or a vessel and immediate assistance is required due to an inadequacy of resources, knowledge, experience, or any combination of these factors. In general, distress situations may be grouped into three categories:
malfunctioning of the ship, e.g. threats to integrity of the ship, engine failure, flooding and fire
medical conditions, such as injury or illness
seafarers falling overboard
The maritime context may influence the urgency of the distress situation. For example, an engine failure occurring close to shore in heavy weather may result in more serious consequences than would the same occurrence on a calm day on the high seas. In reverse, a particular medical condition may be constitute a more serious threat to health when evacuation options are long or access to evacuation assets is unreliable. Thus, situations that may be easily managed ashore may constitute a distress situation at sea, due to limited resources, knowledge, experience or access to external support.
What is maritime search and rescue (SAR)?
Maritime search and rescue (SAR) refers to a wide range of medical and logistical measures that aim to ease or resolve potential or actual distress at sea, and prevent the loss of health and/or the loss of lives. SAR operations include searching for and recovering those who have gone missing, assisting those who are injured or sick and evacuating individuals in needs to a place of safety.
Maritime SAR may draw on all available assets in the area of maritime distress. Assets may include private and public actors including:
vessels afloat in the area including regular merchant ships, military vessels or designated SAR vessels,
airborne assets, such as helicopters, airplanes or drones and
land-based assets, such as the national or regional maritime rescue coordination centres (MRCC) and medical treatment facilities, provisional evacuee reception centres, next of kin information centres, call centres and so forth.
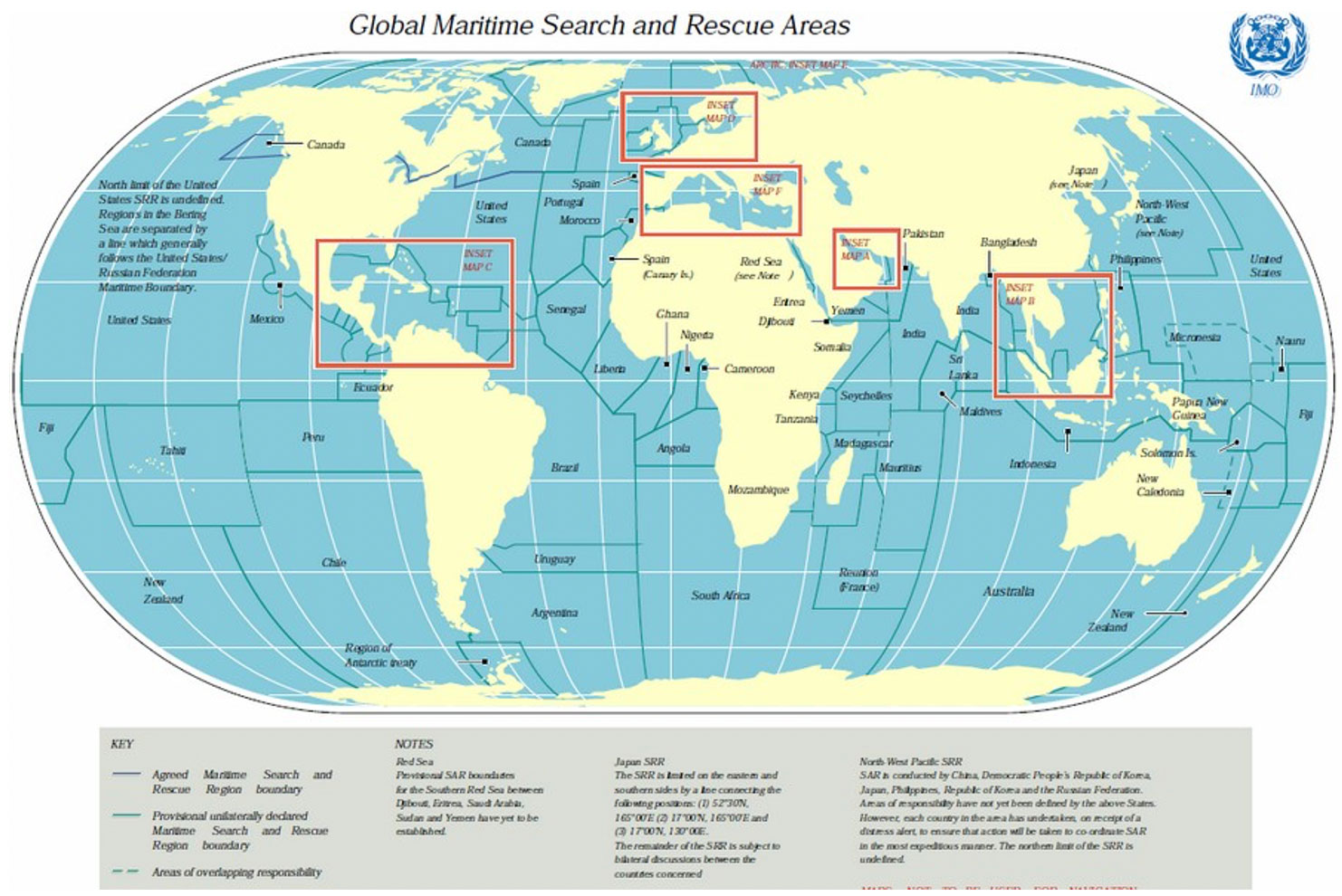
Organisation of SAR services around the world
The SAR Convention of 1979 divides the seas into 13 geographical search and rescue areas, in which coastal states are responsible for coordinating search and rescue through a maritime rescue coordination centre (MRCC). Search and rescue is the responsibility of the coastal states and should be offered to the best of their abilities to anyone in distress in the search and rescue areas, regardless of the national origin of the seafarer, the flag of the ship or the circumstances. Nonetheless, despite a legal framework providing for a complete coverage of geographical responsibilities for search and rescue, many sections of the high seas inevitably remain remote. Thus, the SAR-convention is no guarantee that there will be any actual rescue assets available in an area of maritime distress.
Responsibilities of the coastal state
KATINKA SVANBERG
Coastal states and the individual seafarers share responsibilities for search and rescue, according to international law. Every coastal state shall promote the establishment, operation and maintenance of an adequate and effective search and rescue service.
Under the SAR Convention, a coastal state shall receive the notification of a person in distress and that coastal state would then assume the lead in the search and rescue mission, usually through its coastguard, together with the flag State of the ship.
The national regulations of several states require medical staff to be included in any search and rescue mission. In addition, a ship that conducts a rescue mission must be prepared for its Medical Officer to provide medical treatment to the survivors and to ensure the provision of hot food and drinks.
Operational challenges
SAR services face many challenges in conduction operations. These include
Time and climate. These are often critical in survival of distress at sea. When climate is harsh, the time limit for timely rescue may be dramatically reduced. This relationship is often referred to as the “Arctic delta”, and implies that similar circumstances may involve different sense of urgency of in the Arctic than elsewhere. In order to meet the maritime challenges in the Polar Regions, the Polar Code, detailing additional demands for ship construction and survival equipment, was adopted by IMO in 2014[7].
Political issues. These may also challenge maritime SAR. Piracy and terrorism at sea may hamper maritime SAR efforts. Furthermore, individuals being rescued may be refused entry into a coastal state, the coastal state may not be safe or the coastal state may not be able to provide adequate health services to the seafarer.
Passenger vessels in distress may prompt mass rescue operations. Mass rescue operations may be defined as operations in which rescue capacities are overwhelmed. Constraints to rescue capacity may relate both to the quantity and quality of rescue assets available and to the number of rescue assets that may operate safely at the same time.
When To Stop Searching
KATINKA SVANBERG
If the missing persons cannot be found during the search, the question of when to stop the search for survivors will arise. There is no definite time limit in which a SAR mission should be completed, only that there should be no hope of survival.[8]
This can lead to conflict between the coastal State and families of the missing who may, understandably, want the search and rescue to continue. Such conflict occurred when a cattle ship, The Gulf Livestock 1, capsized in a typhoon in the East China Sea off the coast of Japan in 2020. The 140 metre vessel, with an international crew of 43, and carrying 6000 cows, issued a distress call on 2 September, when it capsized after losing engine power in the stormy weather. Japan’s coast guard raced to find seafarers but heavy winds and rain from the typhoon slowed the initial rescue operation. Only 3 survivors and one fatality were found. One further casualty died in hospital after being found floating unconscious two days after the rescue mission started. On 9 September Japan decided to end the search with 36 Filipino, 2 New Zealanders and 2 Australians still missing. The decision to stop the search came after several days during no additional survivors or signs of the vessel were spotted. The Australian families pleaded with the Australian government to continue searching, but the Australian government announced that this was a responsibility of the coastal state according to the SAR Convention. After failed attempts at seeking Australian Governmental assistance, family and friends of the two missing Australians launched a private rescue mission funded by donations at a cost of approximately 10 000 AUD per day. Still, after three months, no one was found.[9]
[8]Annette L. Adams, et al., Search Is a Time-Critical Event: When Search and Rescue Missions May Become Futile, Wilderness and Environmental Medicine, Vol 18:2, 2007, p.95 -101, p.100.
5 [9] Emily Consenza, Families will never give up hope of finding missing crew members one month on from Gulf Livestock 1 sinking, The Australian, Oct.9, 2020.
D.10 Healthcare of seafarers in ports
Details
ROB VERBIST
Port healthcare
Introduction
Port healthcare is a niche in medical practice. The proximity of a port, ships and those on board leads to specific demands on health care.
Port clinics are often part of a
General Practice clinic near a port
Occupational Health service within a port
Institute of Tropical and Maritime medicine, or a
Travel Clinic.
This depends on the kind of medical service that is most needed in an area, both by the port itself, the industry and the seafarers and passengers coming into the port by ship.
The practice of port maritime medicine demands specific knowledge and skills. It is not a recognised speciality in medicine and encompasses many different aspects of medicine. It needs an organisation and structure that meets the needs of the seafarers as patients or clients and the industry they work in. An all-round port clinic combines aspects of general practice, occupational medicine and tropical medicine, and may include a telemedicine service for care at of the patient form a distance.
The vulnerability of seafarers
Seafarers on board ships are among the most isolated people on the planet regarding access to medical care, both for primary care and in case of an emergency. On a large, slow merchant vessel, in the middle of the ocean a seafarer may be several days away from qualified medical services. In the interim the officer responsible for medical care provides any necessary care, with advice from TMAS where appropriate, utilising only a limited range of medication and equipment from the medical chest. More information on the care on board is available in other sections of this chapter. If required there may be the possibility of an evacuation but this is not always possible and not without risks. More information is available in Ch.5.9.
Of course, there may be a doctor or other health care providers on board but this is often limited to passenger ships. More information on cruise ship medicine is available in Ch. 2.13
Regulations
The Maritime Labour Convention 2006 (MLC)[1] states that ‘each Member shall ensure that seafarers on board ships in its territory who are in need of immediate medical care are given access to the Member’s medical facilities on shore’ and that each Member shall
give seafarers the right to visit a qualified medical doctor or dentist without delay in ports of call, where practicable;
ensure that, to the extent consistent with the Member’s national law and practice, medical care and health protection services while a seafarer is on board ship or landed in a foreign port are provided free of charge to seafarers; and
are not limited to treatment of sick or injured seafarers but include measures of a preventive character such as health promotion and health education programmes
However, the availability and quality of the healthcare found in ports around the world varies hugely. Some ports may have nothing and medical care must be sought from the general medical facilities outside of the port environment where there may be little or no knowledge of maritime medicine or the needs of seafarers or passengers travelling on board. On the other hand, some ports, such as Antwerp and Hamburg, have dedicated medical facilities within the port environment with a medical service dedicated to the needs of the seafarer and the shipping industry. These may be private practices, tailored to serve the needs of seafarers and shipping, or governmental port health services including clinical care. In other places, such facilities may be available but require a journey out of the port to access such care.
Barriers to health care
To contact or visit a doctor during a voyage a seafarer will initially inform the officer responsible for medical care or the Master. By contract and on the basis of international conventions the
company will most often take care of the costs and therefore any arrangements should be made this way. In most cases, this implies that the Master’s permission is necessary for the seafarer to
get medical advice.
The role of the Master
The role of the Master is complex:
Confronted with a medical request by a member of the crew he will seek the advice of a
medical professional, either by radio medical contact or in the next port of call.
If a medical referral is necessary in a port, he will seek the assistance of the ship owner’s
representative in the port to help him find an appropriate medical practioners or facility. This representative is usually the shipping agent.
The Master’s position is that of the owner’s representative on board, he is first of all
responsible for the safety of the ship, the well-being of the crew and for safe manning. But he is also responsible for the costs incurred.
He will also have to be informed of the decisions taken and the need for additional medical care, restricted duties etc. His responsibility is for the safety of the vessel and the crew and he will need to assess the impact of the outcome on both the seafarer and the ship.
The role of the agent
Port shipping agencies have a relationship with the ship owner on a commercial basis and provide a range of services for the vessel and those on board. However they are usually non-medical and their choice of practioners or facility may be dictated by other factors apart from the medical condition of the seafarer. They will also often be the point of contact with the physician and provide the Master with help in line with his demand, attempting to ensure a proper assessment of the case, a swift response and clear report with regard to the safety of the patient, the ship and the rest of the crew. To do this they may have access to medical information that may be sensitive and should be treated appropriately. Further information on ethics and confidentiality is available in Ch xxx.
The relationship with the seafarer
This reality is the main reason why seafarers very often cannot or do not consult their own choice of doctor for advice but are referred to port medical clinics or a doctor chosen by the company or the agent on the company’s behalf. There is an argument that by signing a contract of labour, the seafarer voluntarily limits his freedom of choice with regard to medical advice with the benefit of not having to bear the financial consequences of any illness or injury he might acquire during the time of the contract. However, this way of working is often surrounded in mistrust for many reasons including but not limited to:
fear of losing their job if they are unfit to work,
concern that their medical condition becoming known to many,
cultural differences,
language issues
A port clinic functions against this background. Medical advice is given to seafarers on direct request of the Master. The port physician works for the patient but on the request of the owner. He therefore becomes part of the work relation between the seafarer and his employer.
The Port Health Physician
As mentioned above the port health physician requires a number of skills, both medical and non-medical. Key to fulfilling his role effectively is knowledge of the patient, usually a seafarer, medicine, and the maritime environment.
Konwledge of the seafarer or patient
There was a time when seafarers came to port physicians with vague complaints and minor
ailments, in fact one could think that often the seafarer was just looking for some
tablets, some reassurance, and the possibility to go to a doctor for free or even to get a
free ride into town. Those days are over. Seafarers have complicated tasks to perform in both operational and managerial functions, they are trained people capable of making judgements and often aim to take decisions themselves. They are better selected and they are in better condition when they come on board. That, combined with the decreased number of crew on board and the shorter stay in port, makes consultations by seafarers less numerous but often more complicated in nature.
The approach to the patient must be empathic and open. Seafarers come to a port maritime physician often with a problem that has occurred on board and with which they have been alone for several days, thinking and often worrying. They may have attempted to self-diagnose and this can lead to many misinterpretations and it can take a lot of time and good communication to get these out of their mind. They may have been unwilling to seek assistance on board and therefore have had the problem for a while, or may have been unable or unwilling to access medical care ashore in previous ports. Hence, the cases that maritime physicians see these days are often more complicated.
The seafarer may need referral for more complex investigation and treatment. In this situation, appropriate arrangements must be made and additional communication with other medical professionals will be required to coordinate the care of the seafarer, his return to the ship or his ongoing stay ashore and subsequent repatriation.
In order to assess whether or not a seafarer can return on board and fulfil their duties the port physician must also have knowledge of life on board, the working environment, the tasks associated with the different positions and the medical care available on board. More information on many of these areas is available in this Textbook.
The physician has to keep an extensive record of cases and there is much time and energy needed for each case. Documentation may be required by many parties, with the consent of the patient, and if the seafarer is to return on board he needs good information and instructions on how to continue treatment and when, where or what complications indicate the need to seek follow up.
Knowledge of Medicine
General medicine
The port maritime physician should be able to work independently with an appropriate level of
competence, using evidence based medicine and with a broad knowledge base covering many specialities. He must be skilled in history taking and clinical examination as there is often not time for additional tests. If further tests are necessary, they must give the most useful information possible and referrals for specialist care should be appropriate and add value. Time is a very limiting factor in patient care and this time-pressure becomes a key element in decision-making.
The port maritime physician gives a patient-centred and community-oriented comprehensive and integral service that is responsive as well as anticipatory and includes treatment, prevention, health education and promotion, help and assistance where necessary. However, a characteristic element of general practice that is less present in the port medical practice, is the continuity of care. Seafarers often use the services on an occasional basis, maybe only once in their seafaring career. This requires special attention with regard to reports and plans for follow-up that may occur in another port. The port physician has to assist the patient on how and where to seek follow-up.
Occupational medicine
In a maritime environment a medical decision will always have to take the specific working and living situation of the seafarer into account. The success of the treatment depends on the conditions on board and the implications such treatment has on the individual seafarer and on the safety of the ship. When the professional circumstances of the patient are of such importance in the medical
decision, occupational medical training is very important for a good maritime port physician.
Not only to have an idea about safety and the ability to continue to work on board, but also to identify aspects of work that may cause injury or disease to a seafarer. Hazard definition and risk management, how to modify work activities and monitor trends in health are subjects that a port physician should be familiar with. More information is available in Ch. 2.5.
Knowledge of so called tropical medicine, expanded to all kinds of pathology common in
other areas of the world but less frequent in the country of the physician, is important.
Vaccinations related to work and travel have to be available in the port clinic and travel
advice that takes into account the specific characteristic of the ship and voyage is
certainly a necessary element of the work in a port clinic.
Knowledge of the maritime environment
Ideally, a port maritime physician should have sailed on board a ship. He has to feel, hear and smell life on board. He should experience the way seafarers live on board and the way they work, note the psychological strain of watch systems, feel the physical strain of some work on board and the monotony in other tasks. At the very least physician should have a good idea about the different tasks on board ship and insight into the functional demands of each task. He should have a profile of each function on board and must know particular hazards for health and wellbeing in each of these jobs. More information on this topic is available in Ch 4.3.
It is also important that the physician understands many of the stressors that exist in both living and working on board. These may include the short passages between ports, the numerous tasks to be done while in port etc.… and the isolation from family and friends, little time off and restricted diet and exercise facilities. More information about life on board is available in Ch xxx.
In addition, the physician must also understand aspects of the shipping industry, its regulation and its operations. More information is available in Ch 4.4.
The Port Health Clinic
Services
Many seafarers remain on board, unwell, worried and afraid, longing to get professional assistance as soon as possible, ideally in the next port of call. In order to best assist seafarers port clinics should provide a wide range of services and should be:
able to assess and manage a wide range of acute and chronic medical problems or other issues
able to access secondary care for further investigation and management of more complex medical conditions
able to provide a wide range of other services including pre employment medical examinations (PEME), vaccinations and diagnostic tests, both laboratory and radiological, among others.
assist in questions of fitness for duty and other work related health issues
This requires a well organised referral system both to and within the clinic and to all kinds of specialised consultations and care if required.
Availability
The availability of a physician and work in a port clinic has to be organised in relation to work in the port. Although work at night and during the weekend may have declined in some bigger ports, activities almost never stop. The port maritime physician should organise his work in a way that maximal presence is possible and ideally provides round the clock availability, seven days per week, 24 hours per day. Generally, this is only possible in an association or in a network of port maritime physicians. It is therefore important that the port clinic organises or participates in a regional watch system for the port area.
A port clinic should have physicians available prepared and at all times ready to go on board a ship to provide treatment or advice, not just to receive patients in the clinic. This may happen alongside or at anchor or even while the ship is on its way to or from the port. This may be physically demanding, for example, boarding a ship from a pilot boat and may take many hours if the ship is still some way out of port.
Location of the clinic
The clinic should be
the easiest way for a seafarer to get medical help on arrival in a port.
nearby and easy to access.
In the evolution to the shorter and shorter stay of the ship in port, the location of the clinic or reception of the seafarers in or nearby the port area is important. A clinic should at least be within easy reach of transport coming from the port area and to a certain extent it may need some visibility in the port area itself.
For ease of referrals, the port clinic should be close to an emergency medical care unit and other specialized medical services. The seafarer will not have the time to take long trips to and from these services. Equally, a port pharmacy in the local vicinity, that understands seafaring and is aware of how to deal with maritime patients, is almost a pre-condition to permit the fast and smooth treatment of the seafarer.
Facilities in the clinic
The reception and waiting room must be clean and comfortable and decorated in a way that the seafarers feel at home. A poster or some leaflets in their language, magazines or even newspapers make the seafarer feel recognised in a foreign port.
Health information relevant to their profession should be available so that seafarers recognise the special focus of the clinic to their profession, leaflets and booklets about health at sea should be available to them, free of charge.
Treatment rooms have to be clean and well equipped with separate rooms for treatment and consultation. Rooms should allow the seafarers to have a private and confidential talk with the attending physician although translation or assistance by a third person may sometimes be very important.
Instruments and equipment necessary are basically the same as in general practice but in view of the many accidents on board a focus on the treatment of small wounds and trauma may be necessary.
Specialist care for seafarers.
The Maritime medical unit
Although general medicine is the basis of port healthcare, it is of the utmost importance to have access to other specialities, often in other facilities. The selection of the service, department or individual specialist to refer a seafarer to should be done on the basis of accessibility of their service for seafarers. Ideally a number of specialists and facilities will have been identified by the port physician and they, alongside the port clinic will form a maritime medical unit with focus on the maritime aspects of the seafarer’s life and work.
It is of the utmost importance that the responsible and treating doctor understands seafarers. For an optimal service seafarers require immediate access to a specialist so a rigid appointment system is therefore not good. In reality many specialists who provide this extra service have a link with seafaring, the port, or the maritime world.
Some of the specialities that are most important to have easy and rapid access to are:
Radiology particularly ultrasound,
Orthopaedics and Trauma
Ophthalmology
Dermatology and
Dental care is also critical for seafarers and although dentists often have their own port service it is most important for the port physician to be familiar with that system and to know how to access urgent dental care.
Hospitalisation and ongoing care of seafarers
Whenever a seafarer is hospitalised the maritime physician should closely follow-up the case and actively participate in the process of diagnosis and treatment, making sure that the necessary care is given but also no more than the necessary care.
The role of the maritime physician is to bring up elements of interest for the diagnosis and treatment that relate to life on board and the particular history of a patient. He has to make sure that the hospital specialists and their assistants get background information on the patient and their living and working environment.
The port physician can usefully take an intermediate position between the hospital care and all
agencies and individuals that take an interest in the health of the seafarer and assist in helping the seafarer to get back on board or to get the home as safely and quickly as possible.
Managing the ongoing care of a seafarer landed into a port also involves the
Guarantee of payment for or pre-payment of the hospital costs. It is advised that appropriately trained staff monitor the treatment and costs incurred, in order to ensure that care is appropriate and necessary. This may be the port physician, the agent on behalf of the shipping company or insurer, or an assistance company.
Liaison with the patient, his employer/manning agent/insurer and next-of-kin while he is in hospital. Care must be taken to ensure medical confidentiality.
Practical support of the patient in terms of basic needs and to ensure communication etc. to family and friends. This is often done by the agent but welfare centres and other organisations may play a role.
Arranging for repatriation home back home once the treatment in hospital is complete or a further evacuation for a higher standard of medical care if required. This may involve many different people with different interests and good communication and coordination is vital. More information is available in Ch 5.11 (Repatriation)
Patient management strategy
Introduction
Time is a critical element in medical care for seafarers and therefore it is of the utmost importance to organise an efficient care strategy.
From process-analysis we now understand and use the term ‘critical path’. For medical practice this is called the ‘clinical path’. Such a clinical path is the result of the collaborative effort of many to determine what might be the best way to treat the seafarer.
A clinical path, patient care strategy is built on a quality-first attitude that includes steps to:
Analyse the different steps in a process of diagnosis
Try to find time consuming elements
Try to improve efficiency and quality
Select methods that give faster and more accurate information
This should be done for the more frequent types of care that seafarers need. But the introduction of a path-based management may be easier if it is first applied to types of care where problems are encountered frequently. A good knowledge of a seafarer’s life and likely medical problems is necessary to start this analysis. An example is given below.
The possible clinical path of a seafarer patient
Reporting of the problem on board
This first step in the process is already problematic. A seafarer on board may be in a position that he
does not want to report his problem, for example, because of a poor social protection system, a conflict with a superior, or fear of losing his job.
Permission of the Master to send him to the clinic / hospital
Some Masters do not want to send their crewmembers on land. They think the seafarer is using the
complaint as an excuse to get off the ship for a few hours. They need all hands on deck for work to be done in the port. They may have too limited medical knowledge to judge the situation.
Transport / Access to the clinic / hospital
In a big port, the clinic or hospital may be far from the ship. Often taxis have to take the seafarers and that may take a long time. This may contribute to valuable time lost in the treatment and management of the patient. If the transport service has not been instructed properly they may take the patient to any doctor or a hospital which does not have knowledge of the seafarer’s condition.
Reception
It is of the utmost importance that a seafarer is well received in the clinic. The reception must give the patient confidence with regard to the care he is expecting and language barriers should be handled with patience. An accompanying person from the ship to help with translation is sometimes necessary. The reception staff need to be trained to recognise urgent cases and inform the doctors.
Waiting time
Waiting time should be short in relation to the pathology or the schedule of the vessel. Appointments are good for routine consultations but there should be room for an emergency or an urgent onsultation if the ship is about to depart.
History taking and communication
Always take the cultural background of the seafarer into account. For some it is impolite to givenegative answers or deny. Some have different attitudes towards pain. Always give the patient thechance to express his worries or anxiety.
Clinical examination
Although this is not usually hindered by language problems, it may happen that the response to a est is different because of cultural behaviour. It may also be delicate for some to have to undress nd they may want chaperones to be present. Any uneasy situation may lead to omission of mportant aspects and information. The patient must feel confident and respected.
Laboratory tests
In the selection of an appropriate laboratory test the choice does not only depend on the ifferential diagnosis but also on what can be done before the ship leaves. Relevance of the lab test is mportantbut also more exceptional or ‘tropical’ pathology should be reminded.
Medical imaging
In this respect the selection of the most appropriate test is important, a method that issufficiently sensitive and specific to support the clinical findings and differential diagnosis.Sometimes an ultrasound may give a better chance of obtaining the relevant findings than a CT scan or MRI, sometimes precious time is lost by first doing an ultrasound if in the end an MRI / CT is necessary, etc..
10Communication of results
All results should either be in English or in the native language of the seafarer. If not, an English summary of the reports should be added to the seafarer’s documents. All results should be typed, and written notes are to be avoided. Services that cannot provide immediate protocols of this kind should not be used.
Assessment
It is not unusual in a primary care setting not to come to a diagnosis. Most conclusions are working hypotheses. It is essential and sometimes enough to advise the seafarer about his capacities and risks with the safety of the ship as important reference. He should be advised of things to look out for and how, when and where to seek appropriate follow up.
Explanation
As in every consultation it is a critical to explain the findings and summarise the plan and treatment. Information can be misinterpreted, the seafarer can get lost in technical details or can be frightened by the medical language. Make sure the ideas, concerns and expectations of the seafarer are clearly identified in the history and well explained at the end of the consultation.
Reporting
Reports sent to the ship should hold essential information about the duty status of the seafarer and the safety of the vessel. If the seafarer has to be repatriated or hospitalised it may also be necessary to involve the agent, the company, the insurer and the consulate. Medical and sensitive information should be handed over to the seafarer only and all results of investigations including x-rays are to be given to the seafarer to allow follow up and avoid repeated tests in other ports. In general, the rules of privacy, confidentiality and professional secrecy apply as in any medical activity. More information on this is available in Ch 2.9. The officer on board responsible for medical care may however participate in the treatment and become part of the confidentiality on the condition that they respect the rules. Sharing information with persons not involved in the treatment is not possible.
Medication
Medication has to be given with an explanation in English or the native language of the seafarer. This should include information about dosage, length of treatment and possible side effects, how and where the medication should be kept and how and when to use it. Reports and instructions should always mention the generic names. Pharmacies that can deliver on board are preferred and the seafarer should never pay for the medication, in the first place, the agent, the captain or the insurer should handle this.
Transport back on board
Convenient transport back to the ship should be arranged and assist the seafarer until he is back on board. The transport provider may accompany him to explain further arrangements and follow-up consultations or wait at the gangway to get the seafarer back off the ship to the hospital or airport if appropriate.
This example highlights a number of essential moments and events in a normal consultation that may be decisive for the quality of care a seafarer gets. A real maritime medical service or port clinic is organised in a way that these elements are taken into account and maximal effort is made to overcome the barriers for the seafarer. This can only be done if all partners have knowledge and insight in their roles and tasks from the taxi driver to the receptionist, the nurse and the doctor.
Other health related organisations in ports
Welfare organisations
Very often seafarers are reluctant to trust the port maritime physician because they think they might have links to the Master, the agency or the company. Therefore a seafarer sometimes does not
report personal and more delicate problems for treatment.
Good contact between the port clinic and the welfare services for seafarers in the port is very important so that seafarers that report such issues to the welfare workers/ship visitors get proper treatment and do not lose their rights.
Welfare organisations also play a very important part in visiting hospitalised seafarers and there should be a system to report hospitalisations to them. Often a team of volunteers will visit the seafarers regularly in the hospitals, to offer them newspapers or a telephone services to reach their families.
Sports activities in ports are organised by welfare centres and seafarer’s clubs and medical
support for these activities is important. It should be provided by the port physician and include some guidance and a small medical chest for first aid.
More information on the role of welfare organisations is available in Ch 3.8 and 4.6.
Port Authorities
Because a port maritime physician is operating in their area the port authorities should be aware of the activities in the port clinic. Permission may be needed to enter certain port areas, to go on board ships and to enter specific installations like locks and terminals according to the appropriate rules.
Even if the port clinic is a private initiative the port authority should know about the activities and services given.
In case of a major health problem in the port, the port clinic may be asked to help and
assist in a specific task. It is important to be prepared for such actions and have regular updates and meeting with public health, port health services and port authorities.
Port Health Authorities
Port health authorities are often part of or work closely with port authorities. There main roles are:
Inspection / deratification. Port Health Authorities have the duty to control the ships and port area as regards hygiene and the presence of infections or vermin. They have the authority to fine or detain ships if required.
Control of outbreaks. The port clinic is often the outpost for this service and can be the first to detect an infectious disease on board. Examples include a case of open lung tuberculosis or a positive test on COVID-19. Close collaboration with the Port Health Authority is necessary in these circumstances to organize further examination and care and reduce the risk of further propagation of the infections. Further information is available in Vol VIII.
The port health authority also handles vaccinations and controls the vaccination cards where necessary. In some ports the vaccinations are given by port maritime physicians and therefore a close relation with the port health authorities is necessary.
Maritime Declaration of health. The International Health Regulations, 2005[2] apply to ships and ports and the port health authority ensures/enforces the application of the rules. Every port maritime physician should know these rules and assist the public health authorities to apply them. Further information is available in Vol VIII.
Disaster planning. Ports are very complicated areas when it comes to goods and chemicals stored and handled. In the case of a fire or an explosion, the Port Health Authority is at the core of the rescue planning.
Emergency services
Emergency medical centres in or around the port area should cooperate with port clinics and port maritime physicians. Procedures and protocols may be installed to allow a good communication between these services and the port clinic. Should a seafarer be brought to such a centre directly, the port physicians must be informed about it and contacted to organise follow-up and further care.
A system could be that in such cases the emergency centre is responsible for the
diagnosis and instigating treatment, but that the port physician is involved in writing a report for
the seafarer and ship and has input into the decision on duty status and eventual disembarkation or repatriation of the seafarer because of their knowledge of the work on board and the specific demands for each task on the ship.
Fire brigades and the providers of ambulance transport in the port are also most important partners to locate, rescue, evacuate and transport injured seafarers. The port maritime physician has to keep good relations with these services to find a seafarer who has been evacuated to a hospital urgently.
Maritime Rescue Coordination Centres
In case a ship has announced a medical problem before arriving in the port through the Medical Declaration of Health (MDH), or asks for immediate assistance by a doctor on arrival, it is very important that maritime rescue coordination centres (MRCC) are aware.
They can give the ship priority to enter the port and if necessary they can put it in a special quay or berth for easy access. The centre can advise the doctor and emergency service on the exact time
and place to go on board. Also in case of departure with a medical case that is not finished or if it is necessary to put the seafarer back on board at the last minute, the coordination centre may give important information about the exact time of departure, possibilities to put the seaman back on
board in the locks etc.…
Hospitals
Not many ports have a special harbour hospital or a service for seafarers only and
the port maritime physician should carefully select the hospitals and departments to
cooperate with for specific cases. The geographic position of the hospital may be important not only in respect of the port or the ship but more in relation to the agencies and the welfare
centres so that they can visit a hospitalised seafarer regularly.
Universities
Some departments of a University Hospital may be of importance for port maritime
physicians. The department of Tropical Medicine for example is very important and particularly useful in some cases. The department of the University Hospital where a seafarer is eventually hospitalised should again be briefed about the special procedure for seafarers by the port maritime
physician. Close relationships with such facilities can be beneficial for all.
Port Clinics in other ports
When a seafarer is sent back on a ship he should carry a report including all results and technical documents concerning his examination and treatment and a clear instruction to contact a port physician with these results in hand in case it is necessary. All printed material of a port clinic should mention something like ‘In case you consult a doctor in another port about the same problem, show him all results you have got from us…
Medical records
Electronic patient files
An electronic patient file system should be used that works well with a database that has a large number of files but contains relatively small bits of information. This should all be compliant with data protection regulations, such as the European General Data Protection Regulations (GDPR), including a separate invoicing system in case the payment system for the seafarers is different from the national health system. Regular back-up systems and data security are necessary, as are separated access rights for different functions in the clinic.
Electronic files have the advantage of being portable and allow population analyses. Information should therefore be stored in a standardised way and port maritime physicians are to be encouraged to use, for example. ICPC2 (WHO International Classification of Primary Care, 2nd Edition) to write down their assessment or diagnosis of a case. Even if the files have the purpose of diagnosis and treatment, data may be used for research if they are organised in a correct way and this is an important point at the setup of the systems.
Medical information
All medical information should be handed to the patient and is his property and responsibility. He should keep them safely as he may have to use them in another consultation.
Copies of the report and the result are to be kept in the medical file of the port medical service. Other interested parties like insurances, representatives of the company etc should given information as necessary and as allowed by national regulations etc and with the consent of the seafarer. More information on ethics and confidentiality is available in Ch 2.9.
The medical records should contain:
Identification of the patient
Name and First name
Date of Birth
Nationality
Gender
Rank on board
Identification of the Vessel
Name of the ship
Type of ship
Information of the voyage: trading area, cargo, next port, time in port, estimated time of departure.
Shipping Agency and phone number
Transport company to the vessel and phone number.
Quay, name or number
History of the present illness / injury
Objective findings
Specialized examinations or test results
Assessment
Planning
Treatment
Duty Status
The duty status should indicate if a seafarer is fit with regards to the work he can do on board. Is he completely fit? Completely unfit? Can he do limited tasks? What tasks? Be as specific as possible.
It should also indicate if it is safe for the seafarer to remain on board. For example, a seafarer with a complicated bandage may be able to perform watch duties, but in case of an emergency, like an abandon ship alarm, this man would not be able to save himself and would depend on others. Such reason may be enough to sign him off and repatriate him. This decision must be made in the context of type of ship, kind of voyage and also social network of the seafarer.
Medical report for the Master
Information in this report should allow the Master to judge the condition in a way that he
can evaluate the risk of keeping a seafarer on board and also can estimate the abilities of
the seafarer to return to work. It may also be necessary to report whether a condition holds a risk for the rest of the crew, for example, in case of infectious disease. In that case, a further instruction how to handle the case has to be added to the report.
 If the medical situation of the patient allows and the distance towards a suitable shore-based medical facility is within acceptable reach in distance and time, the safest and most comfortable mode of evacuation is often by the vessel itself delivering the patient. This may imply that the vessel changes its course/ itinerary towards a nearer port than the one that was scheduled. Arrangements will need to be made for appropriate land transportation to meet the ship and for appropriate receiving care for the seafarer. The TMAS doctor, the vessel’s shipping agent or MRCC/JRCC may be able to assist in this.
If the medical situation of the patient allows and the distance towards a suitable shore-based medical facility is within acceptable reach in distance and time, the safest and most comfortable mode of evacuation is often by the vessel itself delivering the patient. This may imply that the vessel changes its course/ itinerary towards a nearer port than the one that was scheduled. Arrangements will need to be made for appropriate land transportation to meet the ship and for appropriate receiving care for the seafarer. The TMAS doctor, the vessel’s shipping agent or MRCC/JRCC may be able to assist in this. The risks of transferring a patient from one vessel onto another at sea must not be underestimated. Even if the sea is calm, walking down the gangway for a sick or injured person, and stepping onto a smaller vessel always has its potential hazards, regardless of the willing help offered from all sides. If the patient needs to be transported on a stretcher, this stretcher will need to be lowered by ropes down the side of the vessel, or via side doors if they are available, to be landed on the deck of the smaller craft below. In cargo ships the deck may be as high as 12 metres above the level of the sea.
The risks of transferring a patient from one vessel onto another at sea must not be underestimated. Even if the sea is calm, walking down the gangway for a sick or injured person, and stepping onto a smaller vessel always has its potential hazards, regardless of the willing help offered from all sides. If the patient needs to be transported on a stretcher, this stretcher will need to be lowered by ropes down the side of the vessel, or via side doors if they are available, to be landed on the deck of the smaller craft below. In cargo ships the deck may be as high as 12 metres above the level of the sea. Helicopters involved in the evacuation of a seafarer from a ship maybe part of the national SAR capability, eg the Norwegian Coast Guard and the United States Coast Guard. These helicopters are manned with a doctor, intensive care nurse or medic who are well trained in medical emergency treatment and transportation. This implies that in getting help from a helicopter to evacuate the patient, expert medical personnel are also available offering a higher level of medical care, all be it in the relatively confined space of a helicopter. The helicopter and its crew will also bring in advanced medical equipment such as life-support and monitoring equipment and a defibrillator. However, in other areas of the world the helicopter and crew used may be a private provider with little or no experience of or training in maritime operations, no medical crew on board to offer care to the patient in transfer and no additional equipment. They are simply a means of transportation. In other areas there may be no helicopter evacuation capability at all, or a very limited number of craft serving a large geographical area.
Helicopters involved in the evacuation of a seafarer from a ship maybe part of the national SAR capability, eg the Norwegian Coast Guard and the United States Coast Guard. These helicopters are manned with a doctor, intensive care nurse or medic who are well trained in medical emergency treatment and transportation. This implies that in getting help from a helicopter to evacuate the patient, expert medical personnel are also available offering a higher level of medical care, all be it in the relatively confined space of a helicopter. The helicopter and its crew will also bring in advanced medical equipment such as life-support and monitoring equipment and a defibrillator. However, in other areas of the world the helicopter and crew used may be a private provider with little or no experience of or training in maritime operations, no medical crew on board to offer care to the patient in transfer and no additional equipment. They are simply a means of transportation. In other areas there may be no helicopter evacuation capability at all, or a very limited number of craft serving a large geographical area.