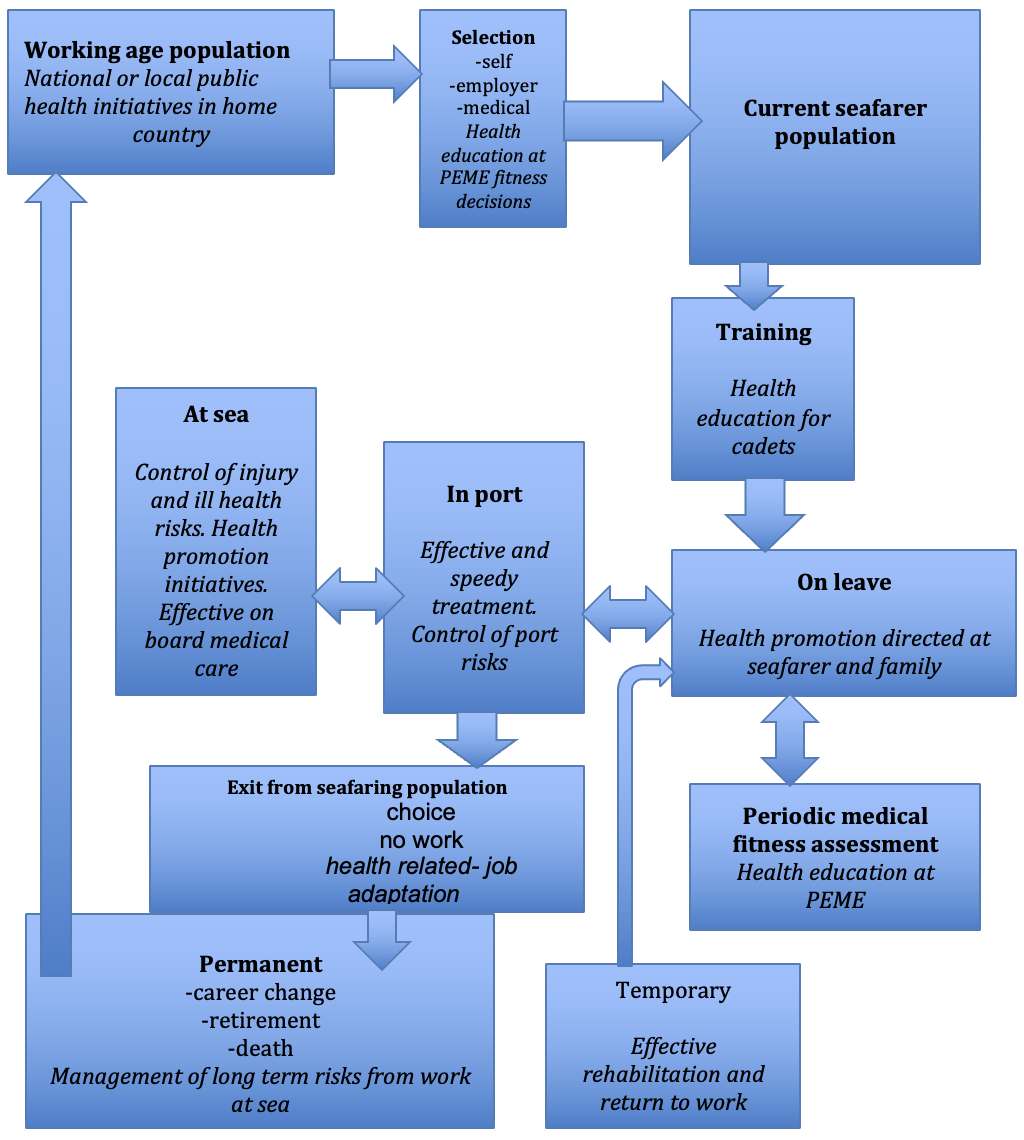
Gaps are considered by reference to the categories listed in Figure 1 in A.3.1
At home
Patterns of ill-health in home country
For some countries there is good information on the causes of illness, injury and death in the local population. Unfortunately, this is lacking or not readily available for many of the major crewing countries. This means that comparisons cannot be made between seafarers and comparable groups in other land based populations in the seafarer’s home country.
PEME fitness decisions at the start of a seafarer’s career and periodically
This should be readily accessible information. There are a number of barriers to analysis, except at the level of individual clinics. Very few maritime authorities or health ministries collect, analyse and publish the findings from statutory PEMEs. PEMEs specified by employers and insurers often collect much more detailed data, but this is usually regarded as proprietary information and analysed for internal use only. It is often also collected and disseminated with little regard to the requirements of medical confidentiality (see chapter 4.8 on PEMEs and 2.9 on ethics)
The at-risk population of seafarers
Military seafarers are state employees from a single country and numbers, jobs and demographic information are available. By contrast, merchant seafarers and fishing industry employees are often on casual or other non-standard contracts and frequently come from a range of countries. Few employers hold detailed records and crews are often supplied by agencies. It is difficult to obtain reliable information on seafarer numbers, jobs and demography except at the level of a single ship. This makes the conduct of rigorous studies of the incidence or prevalence of disease or injury expensive and difficult to conduct.
Health information on cadets
Cadets in training at maritime academies provide a ‘captive population’ to study. Investigations of determinants of physical and mental health have been undertaken in this setting. It has the potential to provide more information, at least for officers to be.
On board
Medical log book entries at sea
Most incidents requiring health intervention at sea are recorded in medical logs and the more serious events are recorded in the main ship’s logbook. However there have been few studies using this information. There is scope for a wide range of case series and comparative frequency investigations, but there are limitations on formal prevalence or incidence studies because of a lack of information on the overall at-risk seafarer populations. An exception to this is in the cruise industry, where valid single ship studies are feasible because of the large numbers of crew.
TMAS contacts
A large number of studies have been published on the pattern of contacts with Telemedical Advisory Services. The findings are not very consistent as different national and commercial services have different customs or criteria that determine the pattern of contacts. Communications from ships are not always coherent because of language and other issues. A major problem is the lack of follow up data. This may be because ships that seek advice do not contact the service to provide information on outcomes or it may be because the ill or injured seafarer is referred to a clinic or hospital and there are barriers of medical confidentiality that stop information on outcomes being passed back to ships or to services.
Ashore
Medical referrals in port
Seafarers with conditions that do not require immediate attention are often referred for investigation or treatment during the ship’s next port call. Following attendance at a hospital or clinic, for investigation or treatment, the seafarer may return to the ship, usually with some form of medical report and treatment plan, provided care can be completed speedily and before the ship leaves the port. Alternatiely, there may be a decision to provide further treatment and then either arrange for the seafarer to fly to re-join the ship at a another port or to repatriate them to their home country. Information from port providers and from ships about such cases has not been analysed. Shipping agents and insurers usually handle repatriations and only a limited amount of information on these cases has been analysed, and then it is often not published.
Emergency evacuations
These normally have TMAS support and are recorded in studies of TMAS referrals.
Self-reports of ill health on leave
There is limited information on ill health during leave periods although some may be found in the few available investigations of mid-career PEMEs. Serious illness may well mean that seafaring careers end. Data on this will only be available if the seafarer has come for a subsequent PEME and been rejected, otherwise the seafarer and their health data are lost to follow up.
After employment
Health related reasons for leaving seafaring population
As above, information is available if a seafarer is found to be unfit at a PEME and this is recorded. It is also, in principle, available for deaths and if health grounds are the reason for the formal termination of a seafarer’s employment.
Rehabilitation and return to work
Little information is available in this area. A small number of studies in crewing countries provide some information. In countries with developed and accessible systems of social security, these records can provide such information. However, few studies have been undertaken.
Population of ex seafarers
Details are rarely available, but they may sometimes be found in national statistics comparing death or illness in different occupational groups. Investigations that are more detailed have been reported in a few countries, where welfare organisations provide whole life support and need to assess future demands.
Causes of illness and death in ex seafarers
Data on deaths may be available from national statistics, while pension funds and social security records that have good occupational information can also provide this information. It is also sometimes possible to study particular diseases using the case-control comparison methods summarised in Ch 2.4 on the models for a knowledge base.
A.3.4 Political and ethical constraints
Details
TIM CARTER
Introduction
There has only been a limited amount of investigation into the health of merchant seafarers and those who work in fishing. This contrasts with the long history of investigations into the health of those serving in the navies of the world.
Incentives for health investigations
There are four main groups with some shared and some conflicting interests in the health of non-military seafarers:
Employers of seafarers and their insurers.
Here the priorities are for competent and reliable crewmembers, with minimum health care costs or disruptions to ship operations. Employers are often only interested in short term health problems as employment is frequently for a single period of sea service. They are particularly concerned about medical conditions and injuries that could lay them open to liability claims, either for direct costs or because of health related failures in performance that put the ship and other crewmembers at risk. They may resist studies that they consider are likely to lead to imposed costs or to define new liabilities.
Seafarers themselves and their trade unions.
Their priority is to prevent harm to members, avoid discrimination in employment and ensure effective rehabilitation and return to work after illness or injury. They also aim to secure compensation for those who have been harmed by their work or been ineffectively treated while under contract.
Governmental and international agencies.
Here the prime concern is for maritime safety and for minimising the effects of health problems on this. They may also want to ensure that seafarers on ships of their flag, or covered by relevant international conventions, receive a good standard of care in the event of illness or injury while under contract.
NGOs concerned with the health and welfare of seafarers.
Such organisations are funded by other interest groups or the public, and aim to improve the health and wellbeing of seafarers. Welfare organisations do this by the provision of facilities on board or in ports. Health practitioners prioritise improvements to the evidence base on risks and interventions, while often also providing preventative or treatment services.
These differences in perspective and the associated lack of funding for investigations have inhibited the development of an improved knowledge base on seafarer health. They can also make the planning of any agreed study complex as each group seeks to protect its own interests.
The influence of interested parties on the knowledge base
There are a number of ways in which interested parties can improve the knowledge base in maritime health. These include the following.
Information collected but not analysed.
From the late nineteenth century, most national maritime authorities recorded the deaths of seafarers, mainly for legal reasons. Until more recent times, these records were rarely analysed to look at seafarer risks. The focus of maritime authorities was on maritime disasters and the loss of life associated with them rather than on patterns of illness and injury to individuals. This lack of analysis on personal injuries and diseases does not appear to be deliberate neglect as there were few public demands for such information. However, it certainly avoided both the need to fund studies and the subsequent need to take action on any notable findings.
Evidence needed to make the case for action.
Seafarers encountered medical services in port and clinicians collected a number of case series of illnesses treated. Here there were clear patterns of preventable illness, for instance the continuing prevalence of scurvy in merchant seamen in the 1860s. This information was needed to make the case for quality assurance of the lemon juice supplied to ships as a preventative.
Employers and government were reluctant to investigate the frequency of tuberculosis in British seamen in the 1920s. Eventually pressure by seafarer organisations and the persistence of a few health professionals led to studies that showed a big excess, but these were largely restricted to those who had recently stopped working at sea because of early signs of the disease. The unwillingness to acknowledge this problem was almost certainly because of the cost implications of providing more spacious and better-ventilated crew accommodation.
Short windows of opportunity for investigation.
There were periods where, for political or strategic reasons, the health of seafarers became more highly valued. Norwegian seafarers were the one group of Norwegians who lost their lives in great numbers during the First World War, despite national neutrality. After the end of the war, the Norwegian Red Cross and other agencies took steps to improve the provisions for seafarer welfare and healthcare, while at the same time investigating the nature and scale of need. Further information on this is available in Ch 2.3.2.3. During the Second World War, there were shortages of seafarers to crew Allied merchant ships and this threatened the supply of food and war materials. New employment arrangements were put in place, with improved port welfare. Data on the causes of unfitness was collected and targeted strategies were developed to reduce the frequency of illness. These focused on specific disabling conditions such as malaria, venereal diseases and tuberculosis.
Employers and their insurers keep information secret.
Both are keen to reduce the frequency of illness in their crewmembers. They have used information on the illnesses leading to repatriation to shape programmes for the selection of crew, however they have failed to make the findings from these publically available and have often built a framework of restrictions on employment based on their unverified findings. Further information on the medical selection of seafarers is available in Ch 4.8.
Occasionally employers or states have funded investigations or reviews that aim to reduce risk. In 1911 the British maritime authority funded experimental investigations to determine the best means of identifying those seafarers who could endanger ships because colour vision deficiencies prevented them recognising red and green navigation lights. The findings from this study led to improved methods of testing that reduced risk, while minimising unjustified discrimination and loss of job opportunities.
A.1.2 Limitations and opportunities
Details
TIM CARTER
Introduction
Knowledge about the health of seafarers has developed over the last few centuries. Particular problems or concerns have led to the collection of information and its use to plan methods for prevention. An early example of this was scurvy and its prevention by dosing seafarers with lemon or other citrus juice. There had long been suspicions that fresh fruit and vegetables prevented the condition and a study in the British Navy by Lind in 1747 provided some scientific support for this. It took a further fifty years for the navy to introduce lemon juice as both a preventative method and a means of treatment. It was to be over one hundred years before lemon juice was used effectively on merchant ships. Further information on the fight against scurvy is available in Ch 2.3.3.1. Similar examples can be cited in relation to infectious diseases such as smallpox and tuberculosis as well as for chronic conditions such as arterial disease and noise induced hearing loss.[1]
Quality of information on health risks
The previous section outlines a model for considering the state of knowledge on seafarer health risks and their management. On review of the available studies up to 2011[2][3] , most were derived from information from one of the forms of healthcare contact shown in Figure 1. There is a weak information base derived from rigorously planned prospective studies on seafarers’ health. Such studies have the advantage of defining an at risk population in advance and then following their subsequent patterns of health using pre-set diagnostic criteria. They have formed the basis for many of the most important and definitive findings on health risks, for instance in onshore occupational health.
Specific issues in data collection
The definition of at-risk populations among merchant seafarers and in fishing has been one of the continuing limitations for epidemiological studies in this group for many years. Present day patterns of global recruitment on short term contracts have made this worse and in the fishing sector, non-standard conditions of employment, for instance on a profit sharing basis, make for similar problems. By contrast, the numbers serving on military ships and their demographic details are normally carefully recorded and they have ready access to a good standard of co-ordinated healthcare. This means that from the initial studies of scurvy in the eighteenth century onwards it has been possible to conduct rigorous investigation on health risks in the navies of the world.
However, naval, merchant shipping and fishing populations all share one common problem in terms of risk estimates: they spend their time in three different settings. The risks while at sea, while in port and while on leave are different. Any truly definitive study needs to look at the time spent in each setting and, indeed to look at the fine detail of each seafarer’s activities in each setting. At sea they will be exposed to different risks depending on their job and the trade the ship is engaged in. In port, risks will depend on freedom to go ashore, contacts with diseases, especially infections that are endemic or epidemic there and injury risks from motor vehicles and violence. On leave, they will lead their traditional lifestyle and be open to its associated risks.
To date the knowledge base on seafarers’ health, with the exception of that on those serving in navies, is far from perfect. Nevertheless, it has provided the basis for setting some priorities for intervention within the range of settings where prevention is practicable. (Figure 2).
The effectiveness of health related interventions
Figure 2. Scope for health related interventions in seafarers
[1] Carter T. Merchant Seamen’s Health 1860-1960: Medicine, Technology, Shipowners and the State in Britain. Woodbridge: Boydell Press 2014.
Most of the available evidence on the effectiveness of interventions comes from time trends in frequency of disease or injury before and after such interventions. Just as for risk assessments, the quality of information on the effectiveness of health interventions is complicated by the different settings in which seafarers spend their time (Figure 2).
When an intervention can take place in a single setting, for instance the prevention of on board injuries or the control of an infection in a port area, and the effects are short term, the evaluation of effectiveness is straightforward. However where risks are spread over several settings, for example, those contributing to arterial diseases such as myocardial infarction or stroke, then both the planning of effective interventions and their evaluation are more complex.
This is a particular problem in relation to aspects of mental health, where risk factors may include personality, home circumstances and the demands of work on board and the consequences in terms of distress or ill health are difficult to quantify.
The ideal approach to the evaluation of interventions is a well-designed experimental study, similar to the randomised control studies used to assess the effectiveness of medications. This form of investigation is rarely feasible in the maritime setting and so planned interventions have to use less rigorous methods, such as using different populations of seafarers, some given the intervention and others with no intervention as comparison groups. Time trends before and after treatment are also used, as are natural experiments where studies take advantage of differences in exposure to presumed risks that are found in different parts of the seafaring population. The methods used to assess all forms of intervention are similar to those used when assessing risk: prevalence or incidence rates for the condition being studied. Well defined diagnostic criteria are needed and have to be applied consistently in all groups used for comparison.
A.3.3 Scientific validity
Details
TIM CARTER
Introduction
Any source of information will have some limitations. The better the design of any investigation, the better understood these will be. As noted, most studies to date have made use of information collected for other purposes. This is likely to mean that aspects such as the standardisation of information on patterns of exposure, and on the determination of adverse effects will be less than perfect.
Key tests of validity
There are several facets of validity. Any information or analysis needs to be assessed in terms of these.
Is the data from a population that is representative of the one you propose to assess risk or to specify interventions on?
The ideal is to have information about a similar population of seafarers to the one you are concerned with. If the results come from an ethnically different population they may reflect patterns of ill health from the home country of the study population rather than those for your target group. If they do not include those who have left seafaring they will not provide a full picture of long-term disease. A study based on a single clinic will simply reflect those who attend, it will not take account of any selection factors that determine who is seen there.
Is the data from a large enough sample to exclude effects that may come from chance variations among small groups?
This is termed the ‘power’ of a study and is an important aspect of good study design.
Is the population used to determine the prevalence or the incidence of a condition clearly defined, with details given?
Risk can be under or overstated if the population is not defined. Age effects may predominate if the two populations used for any comparison are not age matched.
Are well-defined diagnostic criteria used to identify the cases that are used to determine prevalence or incidence rates?
If several people decide on these they are likely to differ from one another. Often when available data is used as the basis for studies there will be little or no control over the diagnostic labels attached to each case of ill-health.
If the study relies on the results from clinical, laboratory or psychological tests, are the tests used valid and relevant to the risk you are assessing?
There are many instances of invalidated or poorly quality controlled tests being used to take decisions on risk or to decide on likelihood of future illness. These are discussed in chapter 4.8.11.