FROM SECOND EDITION BY DOMINIQUE JÉGADEN
E.7.1 Introduction
Mechanical vibration is a ubiquitous source of pollution on board ships. Vibration is defined as the variation over time in movement or position of a mechanical system, with an amplitude that is alternately larger and smaller than a reference value. The parameters involved in vibration are frequency of vibration (in Hertz/Hz), amplitude or displacement (m), speed (m/s), acceleration and direction of displacement (m/s2).
Some studies consider impedance, which is the dynamic force to which the structure is exposed over speed (Z = F/v N s/m).
“Jerk” (m/s3) can also be defined as the derivative of acceleration with respect to time.
It is considered that:
- very low frequency vibrations correspond to frequencies of between 0 and 2 Hz
- low frequency vibrations correspond to frequencies of between 2 and 20 Hz
- high frequency vibrations correspond to frequencies of between 20 and 1000 Hz and more.
They can be either continuous or periodic, and can occur randomly or transiently.
There are three types of conditions under which people are exposed to vibration:
- Vibration transmitted to the whole body in all directions;
- Vibration via the extremities, such as the hands, arms or head.
- Vibration transmitted to the trunk via the lower limbs of a standing person, the pelvis of a seated person or the bed in the case of someone who is lying down.
The latter is the situation that is encountered on board ships, and therefore this is the focus of this chapter.
On board ships, personnel are subjected to whole-body vibration (wbv) on all three axes (horizontal, vertical and lateral). Acceleration is generally between 0.006 and 0.6 m/s2 along each axis in response to movements of the ship, and are very variable depending on sea conditions, wind direction and the position of the subject on board .
Given the complexity of the phenomenon, there are no satisfactory threshold exposure values. An evaluation of exposure of individuals to whole-body vibration is given in international standard ISO 2631.
Equivalent acceleration | Annoyance |
Less than 0.3 m/s² | No discomfort |
Between 0.3 and 0.6 m/s² | Slightly uncomfortable |
Between 0.6 and 1.0 m/s² | Relatively uncomfortable |
Between 1 and 1.6 m/s² | Uncomfortable |
Between 1.6 and 2.5 m/s² | Very uncomfortable |
More than 2.5 m/s² | Extremely uncomfortable |
Relationship between various levels of discomfort and equivalent acceleration (ISO 2631-1:1997)
To evaluate the severity of vibration exposure, the acceleration equivalent (aeq) is calculated, which is the effective acceleration value measured at the point of entry into the body along the three orthogonal directions (x, y, z). The acceleration signal is weighted for frequency and direction in order to take into account human sensitivity to these parameters. An equivalent value over 8 hours (aeq(8h)) is obtained by multiplying the acceleration equivalent as measured by the square root of the ratio of daily actual exposure/8 hours.
In 2002 the EU adopted a Directive concerning minimum health and safety requirements regarding the exposure of workers to the risks arising from vibration. This Directive defines:
- a level of exposure action value (EAV) set at aeq(8h) = 0.5 m/s2 over 8 hours. If this value is exceeded, employers are asked to assess and monitor the risks, to reduce vibration levels, to inform and train workers and to arrange health surveillance.
- a daily exposure limit value (ELV) set at aeq(8h) = 1.15 m/s2, above which it is considered that regular exposure to vibration presents such a risk to health that vibration levels should immediately be reduced.
E.7.2 Vibration exposure on board ships
Vibration exposure on board sea vessels may arise from the following sources:
- the propeller (periodic vibration)
- the engine and ancillary machinery (periodic vibration)
- the sea it self (random vibration)
Installation of ever more powerful propulsion systems on ships with high tonnage with a single driveshaft increases the discrepancy between the rigidity of the driveshaft and the flexibility of the ship’s structure. These phenomena have been responsible for increasing vibration exposure on board ships. If two sources of excitation are close in frequency, a beat phenomenon emerges, and the frequency of this beat is likely to cause a resonant response.
Structural factors
On ships, there are structures that resonate with forced vibration, for example:
- the entire driveshaft, which is liable to respond laterally or longitudinally to excitation from the propeller or propulsion system, and thus in turn excites the structure of the double bottom;
- the entity made up of a diesel propulsion engine and the structure of the double bottom that supports it. This entity responds to excitation in the form of forces and movements caused by the functioning of the engine, and is likely to make the structure of the hull vibrate.
Other “passive” resonators may be excited, such as the deck, partitions, mast, radar equipment etc.
The force transmitted from the propeller to the driveshaft causes vibration, and, in addition, the changes in the wake due to propeller actions, also influences the vibration of the driveshaft and pressure on the hull.
The fluctuations in the wake influences the propeller and the force the propeller transmit to the drive shaft as well as fluctuations in pressure on the hull. If cavitation occurs, the amplitude of pressure fluctuations on the hull will increase.
These fluctuations of pressure are linked to the following:
- variations in propeller thrust: When the propeller provides thrust, the rear of each blade undergoes depression with respect to ambient pressure, and the front undergoes overpressure.
- the number, surface area and thickness of the blades. Pressure fluctuation is a linear function of mean blade thickness and reduces rapidly as the number of blades increases.
- presence of a variable pocket of steam on the surface of the blade and in its wake, as a result of Cavitation is responsible for most vibration problems found on board ships, following excessive pressure fluctuations on the rear underside. Cavitation is equivalent to an increase in blade thickness, and as such causes an increase in pressure fluctuations.
The fundamental frequency of propellers is around 20 Hz for fixed-blade propellers of between 5 and 6 metres in diameter, and 10 Hz for propellers between 8 and 10 metres in diameter.
If the response frequency of the propeller blades is very high (in the audible frequency range), “singing propellers” may be heard. This can be troublesome for the crew.
Engine vibration is caused by alternating piston/crankshaft motion. Excitation caused by free forces and moments within the engine can have an effect on the vibration response of the ship’s structure and even the girder structure, particularly in medium-sized ships with 2-stroke engines.
Engines generally vibrate at between 3 and 30 Hz.
The level of vibration depends, of course, on the type of engine, and particularly the engine speed.
Vibration caused by sea conditions
Vibration of the whole ship:
The swell causes random very low frequency vibration (less than 2 Hz) of the whole ship, both longitudinally (pitching) and transversely (rolling). The frequency of this vibration is between 0.01 Hz in very calm seas and 1.5 Hz in bad weather. It is generally between 0.1 and 0.3 Hz. Acceleration ranges between 0.005 and 0.8 m/s2, sometimes reaching 1 m/s2. These values vary depending on sea conditions and the position of the subject on board the vessel (Kingma) [1].
This vibration causes seasickness.
Ship girder vibrations caused by sea conditions:
These are usually considered to be of two types:
- “Whipping”, which is caused by the hydrodynamic impact to the front of the ship, and which is a transient phenomenon that causes the ship girder to vibrate. Whipping usually occurs when the ship is forging ahead and when there is relative movement of the stem that is great enough to cause impact:
- “slamming”, when impact occurs to a flat part on the bottom of the ship, when it falls back to the sea after emerging.
- “slapping”, which occurs when there are impacts on the flat surface of the stem when it has not emerged from the water.
- large waves (“green sea”).
- “Springing”, which is created by excitation caused by variable hydrodynamic force created by the swell, and which is effectively a phenomenon whereby the ship’s girder is made to vibrate freely.
In conclusion: ships are environments in which significant stress is caused by vibration. Such vibration can be of very low frequency, of low frequency, and to a lesser extent high-frequency (range is between 0.01 Hz and 80 Hz, with a maximum of between 3 and 30 Hz). These vibrations can be periodic or random.
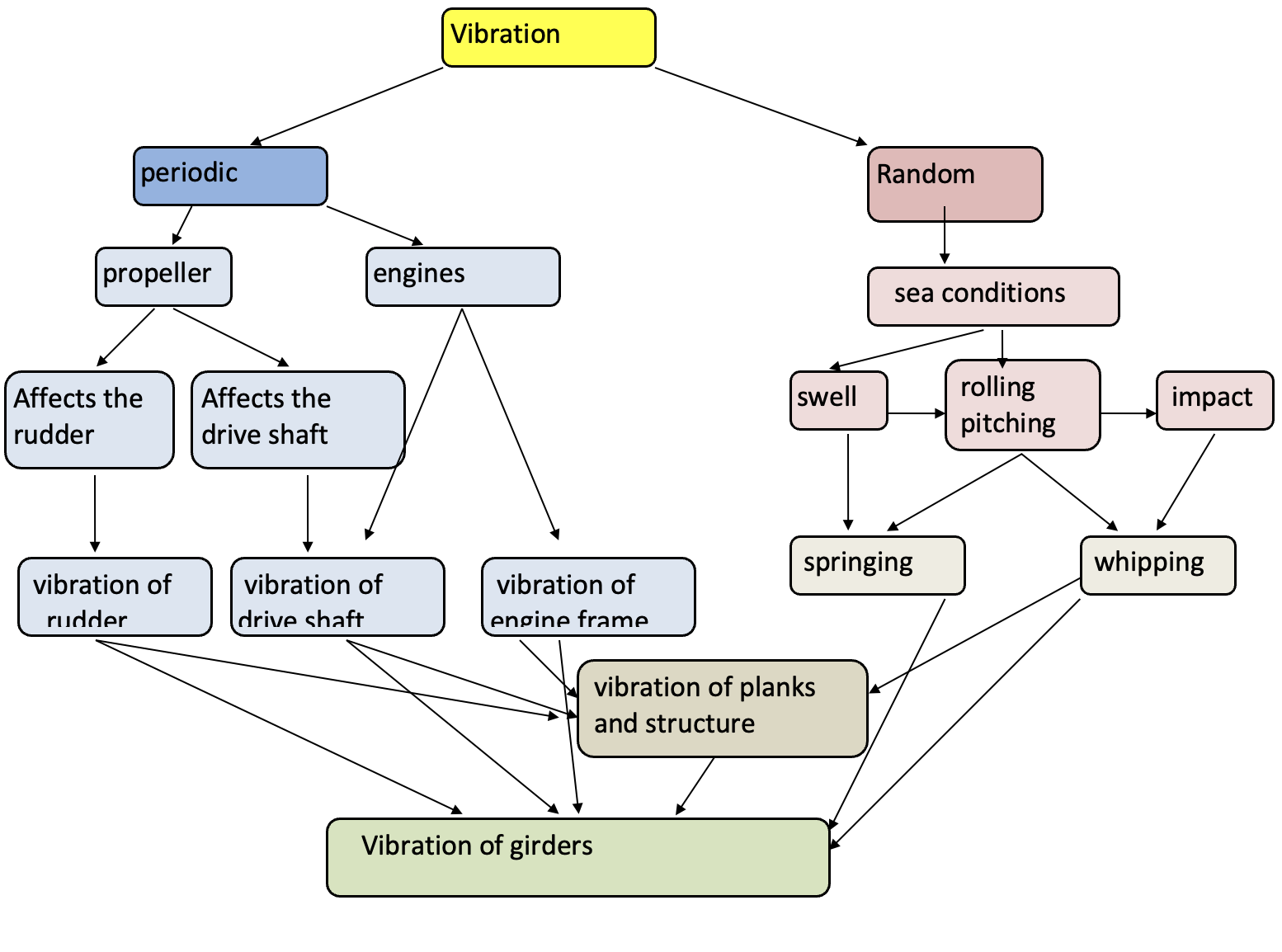
Fig x.x Summary diagram of vibration on board ships
E.7.3 Health effects of ship vibration
Vibration and its effect on the human body.
The human body as exposed to vibration may be reduced to suspended elements (head, thorax, pelvis) linked by shock absorber systems (ligaments, muscles, intervertebral discs).
The physiological and psychological effects of vibrations on humans are caused by significant relative deformation and displacement undergone by organs and tissues at certain frequencies.
The frequency of the sinusoidal movement of a freely oscillating system if it is subject to impetus and not damped is known as the eigenfrequency (or natural frequency). The eigenfrequency of the organ corresponds to the maximum transmission of movement applied to it, if the organ is considered to be an undamped system. (A system with unrestricted motion.) If the system is damped (which is generally the case in the human body), maximum transmission of movement occurs at a particular frequency which is known as the resonant frequency. By definition, the resonant frequency is lower than the eigenfrequency, but there is generally only a small difference between the two, as the organs of the human body generally are not heavily damped.
Some resonant frequencies for a subject who is exposed to vertical vibrations:
- Head: 20-30 Hz. Visual disturbance is also observed between 60 and 90 Hz, which can be explained by resonance of the eyeballs.
- Thorax: 3-7 Hz. This explains the respiratory problems that are observed at such frequencies.
- Heart: 4-8 Hz. Chest pains have been described, which could correspond to heart-related pain.
- Abdominal and thoracic organs: 4 to 9 Hz
- Spine: 2-6 Hz (5 Hz)
- Pelvis: 4-9 Hz
At frequencies of less than 2 Hz, the body reacts like a single mass. In a seated human body, the first resonant frequencies occur between 3 and 6 Hz; in a standing human, there are two maximum values, at 5-6 Hz and 12 Hz (Subashi ) [2].
Resonance occurs when transverse or front-to-back vibration occurs at frequencies of around 2 Hz. It is caused by flexion in the lumbar and thoracic spine, in the hip joints and by curvature of the head.
The perception threshold for vibration is around 0.01 m/s2.
Vibration perception depends on:
- the region and surface area of the body in contact with the source of excitation;
- the intensity, frequency and direction of the vibration;
- the subject’s sensitivity;
- the position and posture of the subject and whether he/she is tense or relaxed;
- the dynamic interaction between the body and the structure via which the vibration is transmitted to the human body;
- the distribution, mass and dynamic properties of any clothes and equipment the subject may be wearing/carrying;
- the environment: noise, temperature, lighting, vision;
- the activity engaged in (physical, mental, visual, oral);
- psychological influences.
A change in posture can alter distribution of body mass and resonance linked to vibration. This can also mean that vibration transmission shifts to another part of the body. The effects may, for example, be different for someone who is standing than for someone who is sitting. Muscular activity can modify the effects of vibration on the organism (Huang and Griffin) [3].
E.7.4 Seasickness (motion sickness)
Introduction
In general, seasickness occurs when there is a conflict between visual information and vestibular and proprioception information. There is a central difficulty in integrating the various sensory messages concerning body movement (this is addressed in Reason and Brand’s “sensory rearrangement theory” [4], or there is a conflict between the inner model and the outer reality.
Seasickness is triggered by very low frequency vibrations (0-2 Hz). Seasickness can be defined as a reflexive autonomic crisis that is linked to movement and that is triggered or worsened by vestibular hypersensitivity, autonomic nervous system irritability or psychological predisposition.
The conditions that determine whether seasickness will arise are the movements of the ship. Frequency and acceleration vary depending on sea conditions and the tonnage of the ship. The frequency of vibration ranges from 0.01 Hz in a very calm sea to 1.5 Hz in bad weather. Acceleration ranges from 0.01 to 0.8g and sometimes 1g. Regular repetition and duration of movement should also be taken into account. A movement that is regularly repeated is more harmful than a sudden, irregular movement.
Seasickness was known as far back as Hippokrates, and the symptom of nausea derives its name from the greek word for boat (naus) [5].
The intensity and duration of symptoms can vary greatly between individuals, depending on the individual and on the type, duration and extent of movement. Especially nausea and vomiting are common in seasickness. Other symptoms - due to autonomic activation - are cold sweating, paleness and increased salivation. More general symptoms include headache, drowsiness, apathy, a vague feeling of illness, anxiety and reduced cognitive performance. Persons suffering from seasickness may be observed as clumsy and off balance, and in pain. There is marked pallor, the nose is narrowed and the blood pressure falls.
There is loss of psychological strength, which is significant and often disabling, with significant reduction in performance, reduction in muscular strength and co-ordination.
At the same time, it is important to be aware that for people in an occupational setting, symptoms may go unrecognized and be interpreted as fatigue or boredom rather than seasickness.
Conditions that increase seasickness:
- Sleep deprivation
- Strong odours: smoke, paint, fuel, perfume, vomit
- Heat
- Confined spaces
- Athmospheric conditions can influence how seasickness develop
- Movement; change of body posture
- Psychological condition: excess emotion
- Contagion: when one person is ill, the people around him/her often are as well
- Apprehension and fear: memories of a bad voyage make seasickness more likely on future voyages.
A recent study has shown that the risk of nausea is at its greatest at around 0.2 Hz (Golding) [5].
Generally, symptoms resolve within the first 24 hours at sea. If the conditions persist, habituation develops relatively quickly, within 72 hours (finding one’s “sea legs”). Some people do not become habituated, and such people are unfit for sea travel.
In exceptional cases, complications arise: examples are dehydration, reduced blood pressure, ketoacidosis.
Pathophysiology of seasickness
The pathophysiology of seasickness is fairly well-known. Balance is a complex system, and information is conveyed by three sensory faculties:
- the vestibular system
- the visual system, particularly as concerns tracking
- the body’s proprioception system, particularly involving the feet and lower neck.
Such information is transmitted to nerve centres in the brain, where they are compared with each other and checked against previously stored information for coherence, which leads to a tailored balance response.
It is certain that seasickness originates in the vestibular system. People who are deaf because of inner ear destruction and animals without labyrinths do not experience seasickness. Very low frequency vibration is within the range of frequencies that activates vestibular receptors. This is not vestibular over-stimulation, but rather a problem with central integration of data that disagree with other receptors, and this causes the symptoms.
Ship roll seems to have a particularly marked effect on the semicircular canals, and pitching affects the otoliths.
It seems as though the central nervous system commits to memory sensory information that correspond to a particular movement situation. If signals from the various sensory receptors are compatible with this internal model, there is no problem. If there is a discrepancy, there are two consequences:
- the internal model is reorganised: A typical example is known as "mal de débarquement" (disembarkment syndrome), which occurs when a subject returns from a period at sea and continues to experience an illusion of ship movement. Symptoms reduce with repeated travel. The occurrence of seasickness reduces greatly with practice. There seems to be a significant correlation between susceptibility to seasickness and mal de débarquement (Gordon) [7,8].Some authors, like Hain [9] and Nachum [10] make the distinction between several degrees of mal de débarquement: « landsickness » between 0 and 48 hours, mal de debarquement (MDD) between 48 hours and one month, persistent mal de debarquement (persistent MDD) if the condition lasts more than one month. The latter condition, which mostly affects women over 40, may last up to ten years. The unpleasantness of the condition can become quite disabling in such cases.
- a sequence of autonomic nervous system effects is begun. Symptoms are caused by the length and intensity of the sensory conflict. O’Hanlon and McCauley [11] and Bles et al. [12] have put forward the theory that only vertical movement causes seasickness (the “subjective vertical conflict theory”), which incorporates the principle that it is the internal representation of gravity that is disrupted when sensory conflict arises. Most sensitivity seems to arise at 0.2 Hz. In an interesting study published in 1998, Wertheim [13] showed that although vertical movement (lift) is a necessary condition for seasickness, rolling and pitching also play an important role. In this study, thirteen men and nine women were exposed to different situations: while the group exposed only to rolling had just one case of seasickness, vertical movement alone caused no cases, but the incidence of seasickness climbed to 50% when the three components were combined. It seems to be head movements, directly connected with the combination of rolling and pitching along with lifting movement, that give rise to the notorious sensory conflict.
Current research on seasickness
Current research into seasickness seem to head in two directions: on the one hand, seeking increased understanding of susceptibility to the condition, and on the other seeking to model the circumstances under which it arises. Although it has long been known that some individuals are susceptible to seasickness, very recent studies have attempted to achieve a better understanding of it. To this end, a questionnaire was developed: the Motion Sickness Susceptibility Questionnaire. Buyuklu et al. [14] report that, in a population in whom this test was administered, 75% of subjects who were defined as being susceptible to motion sickness were prone to seasickness, 90% to carsickness, 10% to airsickness and 5% to simulator sickness, which suggests to me that this test is possibly not ideally suited to a maritime setting. 10% of those who were classified as not susceptible complained of seasickness in extreme conditions. The team also showed that there was a significant difference between men and women, and that women were more sensitive. A fairly recent (2009) study by Meissner’s German team [15] found, for example, that there was a significant difference between cortisol levels and susceptibility to motion sickness in men (not significant) and women (very significant). The second area of research is modelling to predict occurrence of seasickness in various parts of a ship, using impressive mathematical formulae processed using powerful computers. Concepts introduced include MSI (Motion Sickness Incidence), which is the percentage of passengers who vomit within two hours, the formula for which includes vertical acceleration among other variables, and VI (Vomiting Incidence) which is the probability of vomiting among a passenger population. The shape of the ship, its speed, centre of gravity, its moment of inertia, sea conditions and wave directions, the distribution of passengers and facilities on board, are also entered into the formula. Of course, all this comes under the heading of naval architecture, but we should take note of an interesting article by B Haward et al. [16] who studied the emergence of various seasickness symptoms in the crew of a supply boat, taking into account susceptibility to seasickness, ship movement, and also fatigue and sleeping problems. The problems became critical when vertical acceleration (again) exceeded 0.6 m/s2.
Prevention of seasickness
BY ALF MAGNE HORNELAND
Individuals react differently in how susceptible they are to seasickness. Some have history of seasickness that have interfered with their functional ability, whilst others have only experienced mild symptoms not interfering with their performance. Those with a significant seasickness tendency could be offered medication, whilst those with only mild symptoms should be counseled about adaptation to environmental factors.
General advice to all about adapation to the environment[1]:
- Stay midships on lower deck, if possible
- Look at the horizon, or focus on distant objects, if possible
- Be involved with activities of steering if possible
- Avoid reading or looking at a screen
Medication
- Transdermal scopolamine applied behind the ear at least 4 hours before exposure has effect up to 72 hours, when it should be changed if there still is a need. Individuals with persistent symptoms could use a double dose[2]. Scopolamine is generally well tolerated, but could have side effects like sedation, blurred vision, dry mouth, and, in susceptible or old individuals, urinary retention and confusion. Scopoloamine has been demonstrated effective compared to placebo in a meta-analysis[3] .
- Antihistamines have been widely used for prevention of sea-sickness, but they usually cause more sedation than scopolamine. Many different substances have been used, like diphenhydramine, clorpheniramine, cyclizine, cinarrizine, dimenhydrinate and meclizine[4] [5] [6]. Non-sedating antihistamines are not effective against seasickness[7] [8].
- In refractory situations, when scopolamine or antihistamines do not produce the desired effect, promethazine has been used, but not much is published beyond anecdotal evidence. Oral scopolamine could be an alternative, but is not available in all countries. In some cases diazepam or phenytoin have been used with effect.
- Combinations of a sedating antihistamine with a central stimulant (ephedrine, caffeine, and even amphetamine) is possible to use in cases where sedation must be avoided. Several combinations are available over-the-counter.
Treatment of seasickness
BY ALF MAGNE HORNELAND
If preventive measures have not been effective, and symptomatic seasickness occurs, it is a high likelihood that orally given medicines will not be absorbed as normal because of gastric stasis and vomiting. The parenteral route should be used for medication. One should continue to use the preventive measures mentioned above, and in addition promethazine injected intramuscularly or given as rectal suppository could be useful – 25 mg every four to six hours as necessary[9].
E.7.5 Other health problems associated with whole-body vibration (wbv)
Vibration can cause many different symptoms in the human body, like:
- General discomfort and fatigue
- Reduced performance which could lead to workplace incidents
- Musculoskeletal disease
- Low back pain
- Neck- and shoulder problems
- Herniated discs
- Early degeneration of the spine
- Cardiovascular
- Respiratory problems
- Neurological effects
- Endocrine and metabolic changes
- Reproductive organ damage
- Impairment of vision and balance
- Increased nose-related hearing loss as compared to noise-exposure alone
A number of factors can increase the health effects in the human body, like prolonged sitting in constrained or poor postures, frequent twisting of the spine, twisted head postures, cold work temperatures and stress. Workplace design and task/work organization can influence the effects of exposure to whole-body vibration.
FATIGUE AND SLEEPING PROBLEMS
Along with seasickness, Haward et al [16]. have shown that fatigue and sleeping problems are strongly correlated with movement along all three axes, and the strongest correlation is with sleep quality. Hours spent asleep were negatively correlated with amplitude of movement.
On board ships, vibration of between 2 and 20 Hz is found, and as we have seen this is linked to the propulsion system and propellers. The intensity of this vibration is generally quite low. Depending on the RPM of the engine, this vibration can be amplified and, if this occurs, inconvenience is caused to those trying to write or read. This can also cause partitions to resonate, and can generate unpleasant noise which will increase general fatigue and exacerbate concentration problems. Many authors have attempted to quantify the reduction in performance experienced by people exposed to periodic and random vibration. Vibration makes a task more difficult and cumbersome. Vibration hampers precise movement and accurate prehension with hands and fingers.
Vibration also leads to an increase in reaction time, requiring greater concentration on the task in hand at the expense of attention to secondary tasks, which means that vigilance is reduced.
SPINE AND LOW BACK PAIN
Lower back pain is also associated with an increase in amplitude of ship movement. Törner et al. [17, 18] have reported that vertical acceleration of ±0,4m/s² and rolling of ±8 degrees on board trawlers is associated with an increase in cerebrospinal fluid pressure. Hoogendoorn's [19] work suggests that twisting movements of the spine are an independent factor responsible for lower back pain. Such movement is common on board as individuals seek to keep their balance as the ship moves, particularly on board small vessels. However, Törner has shown that knee movement acts as a buffer. In spite of this, compression forces may be increased while carrying materials on board, because of increased contraction when attempting to stabilize (Barzgari) [20]. Several authors (Törner) [18], (Wertheim) [21] have shown that oxygen consumption was increased in subjects standing on board ships while undertaking a lifting task, but that oxygen exchange was reduced, because of overall muscular tension, which increases fatigue levels. Conversely, Drerup [22] found no abnormalities in intervertebral discs in subjects exposed to whole-body vibration, in comparison with a control group.
In a subject who is exposed to this type of vibration, shifting body mass and maintaining posture (particularly in the case of random vibration such as whipping and springing jerks) leads to stimulation of muscular activity which compensates for the effects of vibration. If there are major jerks (acceleration greater than 2 m/s2), there can be trauma to the lower back, in the form of fractures or compression injuries, particularly to L3-L4 (Ayari) [22].
Holmlund et al.[23] have shown that impedance increases as a function of frequency, up to an initial maximum in the 4-6 Hz range, which particularly affects the spine. There is a second and third impedance maximum in frequency ranges 8-12 and 50-70 Hz.
Subjects exposed to medium-frequency whole-body vibration have been shown to have a higher incidence of lower back pain (Burdorf) [24].
Vibration can lead to microscopic trauma of the spine, particularly the lumbar spine, which are particularly troublesome because the spinal column is unbalanced. On board ships, particularly fishing vessels, vibration is a factor that exacerbates problems caused by postural constraints and the difficulty of keeping one’s balance in a moving vessel, as we have seen. The most significant responses were in the 5-8 Hz range.
RESPIRATORY SYSTEM
Low-frequency vibrations, particularly between 4 and 12 Hz, tend to increase respiratory parameters: respiratory frequency, ventilation rate and oxygen uptake (Maikala) [25]. These increases seem to be linked to general muscular tension caused by vibration: at 10 Hz, there is very significant tension in the muscles in the lower back, chest, abdomen and back.
CARDIOVASCULAR EFFECTS
An increase in heart rate is often observed. Between 4 and 11 Hz, when vibration is of significant intensity, disturbances to heart rhythms have been observed, in the form of extrasystoles and at times tachycardia.
Occasional cases of myocardial infarction in young people with no history of arteriosclerosis or coronary artery disease, have been linked to vibration.
DIGESTIVE AND URINARY TRACT
Digestive tract and urinary tract problems have also been observed, which are partly due to changes in peristalsis in visceral smooth muscle.
This all has an effect on general levels of fatigue, which are already raised by various causes (noise, very low frequency vibration, stress etc).
LOCAL EFFECTS – HAND/ARM VIBRATION SYNDROME (HAVS)
High-frequency vibrations, above 20 Hz, have a purely local impact. The most commonly studied example of this is vibrating tools. Some seafarers (engineers or deck crewmembers) are likely to use such tools, for rust removal, sanding and cutting. Upper limb conditions arising from such vibration are well known. High-frequency vibration can cause angioneurotic problems in the hands and fingers, arthritis in the elbows and finger joints, bone disease in the carpal bones (necrosis of the lunate bone or Kienböck’s disease). These diseases are rare in seafarers, but it is nonetheless essential that the field of maritime medicine gain familiarity with them in order to diagnose and prevent them.
E.7.6 Bibliography
- Kingma I, Delleman N, Van Dieën J. The effect of ship accelerations on three-dimensional low back loading during lifting and pulling activities. International Journal of Industrial Ergonomics 2003; 32: 51-63
- Subashi G, Matsumoto Y, Griffin M. Modelling resonances of the standing body exposed to vertical whole-body vibration - Effects of posture. Journal of Sound and Vibration 2008; 317: 400-48
- Huang Y, Griffin M. Nonlinearity in apparent mass and transmissibility of the supine human body during vertical whole-body vibration. Journal of Sound and Vibration 2009 forthcoming,
- Reason JT, Brand JJ. Motion sickness. London, Academic Press, 1975
- com, Motion sickness, literature review current through May 2021.
- Golding JF, Mueller AG, Gresty MA. A motion sickness maximum around the 0,2 Hz frequency range of horizontal translational oscillation. Aviat Space Environ Med 2001; 72: 188-92
- Gordon CR, Spitzer O, Doweck I, Melamed Y, Shupak A. Clinical features of mal de debarquement: adaptation and habituation to sea conditions. J Vestib Res 1995; 5: 363-9
- Gordon C, Spitzer O, Shupak A, Doweck I. Survey of mal de debarquement. BMJ 1992; 304: 544
- Hain T, Hanna P, Rheinberger M. Mal de debarquement, Arch Otolaryngol Head Neck Surg 1999; 125: 615-20
- Nachum Z, Shupak A, Letichevsky V, Ben-David J, Tal D, Tamir A et al. Mal de debarquement and posture - reduced reliance on vestibular and visual cues.
- O’Hanlon J, Mc Cauley M. Motion sickness as a function of the frequency and acceleration of vertical sinusoidal motion. Aerospace Medicine 1974; 45: 366-9
- Bles W, Bos J, de Graaf B, Groen E, Wertheim A. Motion sickness - only one provocative conflict? Brain Research Bulletin 1998 ; 47: 481-7
- Wertheim A. Working in a moving environment. Ergonomics 1998; 41: 1845-58
- Buyuklu F, Tarban E, Ozlioglu L. Vestibular functions in motion sickness susceptible individuals. Eur Arch Otorhinolaryngol 2009; (published online 26 February 2009)
- Meissner K, Enck P, Muth E, Kellermann S, Klosterhalfen S. Cortisol levels predict motion sickness tolerance in women but not in men. Physiology & Behavior, in press 2009
- Haward B, Lewis C, Griffin M. Motions and crew responses on an offshore oil production and storage vessel. Applied Ergonomics 2009 in press.
- Törner M, Blide G, Eriksson H, Kadefors R, Petersén I. Musculo-skeletal symptoms as related to working conditions among Swedish professional fishermen. Applied Ergonomics 1988; 19 (3): 191-201
- Törner M, Almstrom C, Kadefors R, Karlsson R. Working on a moving surface – a biomechanical analysis of musculoskeletal load due to ship motions in combinations with work. Ergonomics 1994; 37(2): 345-62
- Hoogendoorn W, Bongers P, De Vet P, Douwes M, Koes B, Miedema M et al.Flexion and rotation of the trunk and lifting at work are risk factors for low back pain: result of a prospective cohort study. Spine 2000; 25: 3087-92
- Bazrgari B, Shirazi-Adl A, Kasra M. Computation of trunk muscle forces, spinal loads and stability in whole-body vibration. Journal of Sound and Vibration 2008; 318: 1334-47
- Wertheim A, Kemper H, Heus R. Maximal oxygen uptake during cycling is reduced in moving environments: consequences for motion-induced fatigue. Ergonomics 2002; 45: 186-202
- Drerup B, Granitzka M, Assheuer J, Zerlett G. Assessment of disc injury in subjects exposed to long-term whole-body vibration. Eur Spine J 1999; 8: 458-67
- Ayari H, Thomas M, Doré S, Serrus O. Evaluation of lumbar vertebra injury risk to the seated human body when exposed to vertical vibration. Journal of Sound and Vibration 2009; 321: 454-70
- Holmlund P, Lundström R, Lindberg L. Mechanical impedance of the human body in vertical direction. Appied Ergonomics 2000; 31: 415-22
- Burdorf A, Hulshof C. Modelling the effects of exposure to whole-body vibration on low-back pain and its long-term consequences for sickness absence and associated work disability. Journal of Sound and Vibration 2006; 298: 480-91
- Maikala R, King S, Bhambhani Y. Acute physiological responses in healthy men during whole-body vibration. Int Arch Occup Environ Health 2006; 79: 103-14
- Lackner JR. Motion sickness: more than nausea and vomiting. Exp Brain Res (2014) 232:2493–2510
[1] Bos JE, MacKinnon SN, Patterson A. Motion sickness symptoms in a ship motion simulator: effects of inside, outside, and no view. Aviat Space Environ Med 2005; 76:1111.
[2] Bar R, Gil A, Tal D. Safety of double-dose transdermal scopolamine. Pharmacotherapy 2009; 29:1082.
[3] Spinks A, Wasiak J. Scopolamine (hyoscine) for preventing and treating motion sickness. Cochrane Database Syst Rev 2011; :CD002851.
[4] Buckey JC, Alvarenga D, Cole B, Rigas JR. Chlorpheniramine for motion sickness. J Vestib Res 2004; 14:53.
[5] Brand JJ, Colquhoun WP, Gould AH, Perry WL. (--)-Hyoscine and cyclizine as motion sickness remedies. Br J Pharmacol Chemother 1967; 30:463.
[6] Lucertini M, Mirante N, Casagrande M, et al. The effect of cinnarizine and cocculus indicus on simulator sickness. Physiol Behav 2007; 91:180.
[7] Kohl RL, Homick JL, Cintron N, Calkins DS. Lack of effects of astemizole on vestibular ocular reflex, motion sickness, and cognitive performance in man. Aviat Space Environ Med 1987; 58:1171.
[8] Cheung BS, Heskin R, Hofer KD. Failure of cetirizine and fexofenadine to prevent motion sickness. Ann Pharmacother 2003; 37:173.
[9] Davis JR, Jennings RT, Beck BG, Bagian JP. Treatment efficacy of intramuscular promethazine for space motion sickness. Aviat Space Environ Med 1993; 64:230.